‘I’m still not convinced breastfeeding 4 year olds should be considered normal!’ – feedback from final year medical student after teaching session
‘Most [UK] pre-registration training for healthcare practitioners who work with mothers, children and young infants has many gaps in the high-level standards and curricula…’ World Breastfeeding Trends Initiative report 2016
As a consultant paediatrician, I deliver a one hour seminar to our medical students several times a term. I have the coveted before-home time slot for ‘essentials of paediatric nutrition’, which aims to encompass the investigation and management of faltering growth, the aetiology and treatment of obesity, and all infant feeding issues. Luckily I talk fast.
Of course, I’m joking. Covering the syllabus in that time means focusing on key points, and one way I try to do this is encourage the students to set the agenda. At the start of the seminar, I plot out on a whiteboard what they want to get from the session. The students always ask me to cover the different types of formula. In fact, their syllabus emphasises breastfeeding, but their preoccupation is with learning components of, and indications for, breastmilk substitutes. This is manageable rote learning, standard in undergraduate education, easy to put on a flashcard and commit to memory for exams. It also connects to the overwhelming societal perception that formula is the default feed for babies. It is much harder to open up a discussion about breastfeeding and accept that we, as doctors, know almost nothing about it because we aren’t seeing it or learning about it at medical school. Of the twenty or so students in each session, often only one or two have seen a baby breastfed at all. Usually no one in the room has seen a child over the age of one nursing.
The ignorance around breastfeeding continues into our postgraduate curriculum. The ‘breast is best’ message is emphasised (although that has been superseded elsewhere by the ‘breast is normal’ message) but without the backup of grounding in lactation physiology and how our profession contributes to what I think of as ‘iatrogenic low milk supply’ – medical practices such as separating mother and baby, delaying the first feed, not respecting the importance of skin to skin, feeding on an artificial schedule, wrongly assuming that maternal and infant medical conditions and medication preclude breastfeeding… Without understanding the science, doctors will always resort to what they have seen before, are comfortable with, and believe to be normal. At the moment, that is usually formula feeding.
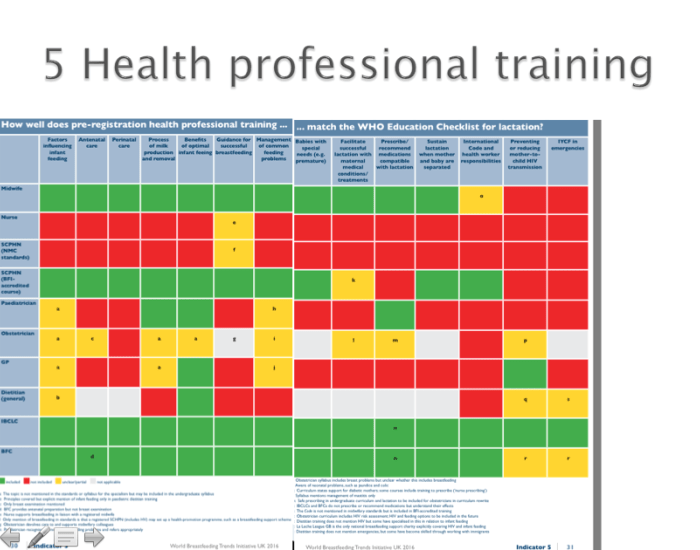
The World Breastfeeding Trends Initiative report flags up the holes in training for healthcare practitioners – illustrated here, the universal minimum pre-registration standards set by the GMC, the NMC and the BDA – and my experience echoes that (see Indicator 5, in Part 1 and Part 2, online). Our doctors need to realise what they don’t know about breastfeeding before they can start to learn. Recognising this is the first step on a very long road, but it is at least a step forward.

Dr Vicky Thomas is a consultant paediatrician at the Great North Children’s Hospital in Newcastle upon Tyne. A generalist at heart, she has developed an interest in growth and nutrition and is passionate about the role of breastfeeding in optimising child health.

Broken link? Can’t read the rest of this post!
>
LikeLike
The postnatal wards are routinely staffed by foundation doctors, gp trainees and a scattering of paediatric trainees. I have seen so much terrible practice, all coming from the best of intentions. Healthy term baby fed after birth then not interested for 5 or 6 hours – e.g. gp trainee did a blood sugar which was borderline and told mum to feed 10ml/kg by bottle (obviously then had to be formula to get that volume). It is just so sad that health professionals are failing families even in the first hours and days of life…
LikeLike