Health professional training needs to include more on infant feeding
Gaps in health professional training on infant feeding have been one of the most talked-about findings of the WBTi project in the UK.
The soft launch of the second WBTi Report on UK infant feeding policies and programmes was held at Guy’s Hospital, London, on March 25th, with a focus on gaps in pre-registration training for health professionals.
The WBTi assessment also includes in-service training. In the UK, the main source is UNICEF Baby Friendly Initiative training.
What were the gaps? Little has changed in these high level universal standards since the 2016 WBTi report. The most striking gap is that the general requirements for all nurses do not explicitly include infant feeding; this means that university health visitor training programs are not required to include much on breastfeeding, unless they are UNICEF Baby Friendly-accredited. Only 21% of university health visitor training programmes are BFI-accredited, although many health visitors will go on to receive in-service training as 69% of health visiting services in the community are now BFI- accredited. Nurses in other parts of the health system, from emergency rooms to oncology or women’s health, and even in paediatric and neonatal wards, have not routinely received training in breastfeeding.
Little support for hospitalised mothers
The WBTi team also conducted a survey of infant feeding leads on NHS Trust policies to support hospitalised mothers who are breastfeeding in wards other than maternity, for example to maintain their milk supply. We found that many Trusts lack such a policy. Scotland does have a guideline that has now been rolled out across the NHS in Scotland.
Sharing our findings
The event was well attended by key stakeholders, including representatives from the Department of Health and Social Care and devolved nations, health professional bodies, UNICEF Baby Friendly Initiative, and members of the WBTI Core Group.
The WBTi Steering Group – Helen, Clare, Alison and Patricia
Dr Bob Boyle of Imperial College set the scene with an historical background of infant feeding in the UK and globally. The WBTi team gave an overview of the report, emphasising the importance of every mother in the UK having access to an integrated network of infant feeding support, and the essential need for political commitment to enable this.
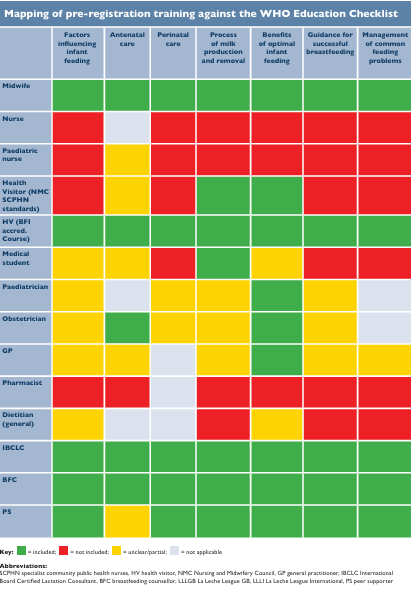
Mapping of pre-registration training standards against the WHO Education Checklist
The UK WBTI assessment maps national minimum standards for training on infant feeding topics against the Educational Checklist from WHO.
The WBTI mapping shows what any family, in any part of the UK, can expect as a minimum from their local health professionals, including not only midwives and health visitors, but also GPs, paediatricians, dietitians and pharmacists.
The assessment found some improvements, but many gaps remain, as can be seen in the chart below, with the red indicating the gaps. It is essential that everyone caring for parents have knowledge of breastfeeding. Health workers should be able to support parents’ goals, and avoid inadvertently undermining their infant feeding decisions.
WBTi summary table of breastfeeding topics in health professional standards
Table of basic standards in breastfeeding topics. More details can be found in Indicator 5 in the full report (Part 1). See Part 2 for a more detailed breakdown.
Author
Dr Alison Spiro is a member of the WBTi Steering Group. She is a retired NCT breastfeeding counsellor, specialist health visitor and hospital and community infant feeding lead, taking both trusts to Baby Friendly accreditation. She completed her MSc in 1994 and PhD in 2004 on Gujarati culture and breastfeeding, doing her fieldwork in Harrow and India.
Alison is the author of a book ‘Breastfeeding for Public Health, a guide for community health professionals’ published by Routledge.
Skilled health professionals are a fundamental building block for successful breastfeeding. Parents expect all healthcare professionals to have the knowledge and skills to help them overcome practical challenges and to offer them emotional support. The reality in the UK is that many have not received the training they need to do this, so parents do not always receive the support they need. While improvements have been seen, UK health professional training still shows gaps in training in infant feeding. Relevant, evidence-based training is needed for all those who work with women, infants and young children.
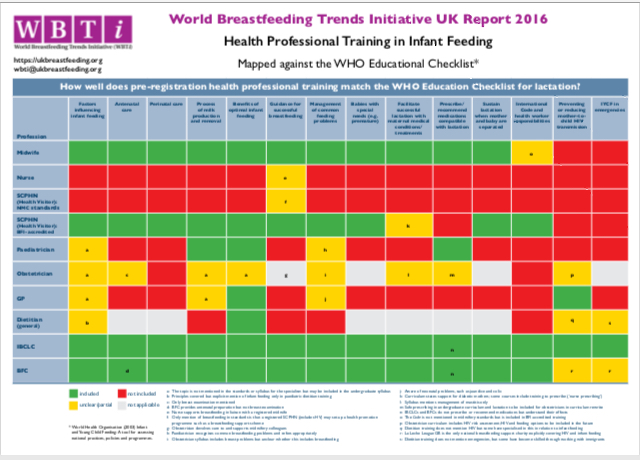
WBTi findings: mapping UK high level health professional training standards in infant feeding against the WHO Educational Checklist
WBTi’s research has found numerous gaps in the pre-registration training in infant feeding in almost all UK health professional specialisms. Only midwifery training covers most of the topics on the WHO’s Educational Checklist on infant and young child feeding.
Alarmingly, the worst gaps are in the high level training standards for nurses, including paediatric nurses. Since the publication of our first report in 2016, there have been a few improvements in the training standards set for paediatricians and GPs, and our upcoming reassessment will be mapping these against the WHO checklist.
What can YOU do?
If you are a health professional,urge your governing body to strengthen the requirements on infant feeding in your professional standards and examinations by:
It takes a village to raise a child – we all have a role to play to support breastfeeding mothers and babies.
We all are the building blocks responsible for supporting new families: partners and family members, health workers, neighbours and community members, religious leaders, employers, academics, governments and policy makers. We can all make a difference. We need to step up to our responsibilities. Everyone needs to understand the importance of breastfeeding – for maternal and infant physical and mental health and wellbeing, for public health, for our economy, and for our planet.
For WBW this year, WABA has produced an extensive suite of materials looking at all these roles and responsibilities. They have outlined the challenges that breastfeeding families face at every stage from conception, through birth, getting breastfeeding off to a good start, and maintaining breastfeeding all the way through starting solids and going back to work, and the solutions we need in each situation – all backed up by links to the latest evidence.
The #WBW2022 Action Folder pulls all this together: it is a useful resource for anyone using evidence to build policies and best practice. You can download it as a PDF and all the links to research and references will be live.
The UK WBTi team will be highlighting just a few of the concepts this week:
Health workers: the importance of relevant, evidence-based. The advertising of follow-on milks, on the media, from 6 months in the UK has led to confusion, resulting in some parents seeing formula milk as equivalent to breastmilk, or that breastfeeding should stop at 6 months. The International Code needs to be adopted by the UK government in full, to reduce this confusion and protect breastfeeding. training for all those who work with women, infants and young children
UNICEF UK Baby Friendly Initiative and the BFHI worldwide sets out ways in which healthcare staff can receive sound, evidence-based, basic training in supporting breastfeeding.
ALSO join a special webinar from the Global Breastfeeding Collective on BFHI, with some added specialist topics on supporting small and underweight breastfeeding infants, and on infant feeding in emergencies. (7-9 AM BST and again at 4-6 PM BST). Register HERE
Community support: Access to skilled, integrated support for all, with a special focus in the GBC webinar on how to support breastfeeding infants who are not gaining well (NICE NG 75,2017). All parents should have easy access to trained healthcare staff- midwives, paediatricians, health visitors and GPs- breastfeeding peer supporters and specialist support (IBCLC, BFCs). Supporting breastfeeding in complex circumstances: Specialist support from IBCLCS, BFCs, or infant feeding leads, integrated with specialist healthcare teams
Protecting infants and young children in emergencies. National policies should guide Local Resilience Forums but these do not exist at present.
The impact of misleading marketing: The International Code. The advertising of follow-on milks, on the media, from 6 months in the UK has led to confusion, resulting in some parents seeing formula milk as equivalent to breastmilk, or that breastfeeding should stop at 6 months. The International Code needs to be adopted by the UK government in full, to reduce this confusion and protect breastfeeding.
Governments with national and local policy makers need to protect all families and support them to make informed feeding decisions free of commercial influence.
What can YOU do?
It is time for a reassessment of the UK’s national infant feeding policies and programmes. YOU could help! Volunteers are welcome with knowledge in any of the ten policy areas (Indicators 1-10), or with skills such as research, writing, graphics, social media and more – feel free to contact us for a chat!
WBTi Key Indicators:
Indicator 1: National policy, programme and coordination Indicator 2: Baby Friendly Initiative Indicator 3: International Code of Marketing of Breastmilk Substitutes
Indicator 4: Maternity protection Indicator 5: Health professional training Indicator 6: Community-based support Indicator 7: Information support Indicator 8: Infant feeding and HIV
Indicator 9: Infant and young child feeding during emergencies
Indicator 10: Monitoring and evaluation
Which one will YOU choose?
Contact us: wbti@ukbreastfeeding.org
Helen Gray MPhil IBCLC is Joint Coordinator of the WBTi UK Steering Group.
How can communities change to give parents consistent support with breastfeeding?
Our Harrow model of integrated working across hospital and community services showed that when professionals, lay supporters and specialists worked effectively together under a shared strategy and infant feeding policy, that more parents felt supported to breastfeed their babies. Over two years higher breastfeeding initiation, continuation and exclusivity rates were beginning to be reported. Parents found that they experienced less conflicting advice and breastfeeding gradually began to be seen as the normal way to feed babies in Harrow.
This was achieved through joint training sessions involving community and hospital staff. Midwives, midwifery managers, paediatricians, neonatal nurses, paediatric nurses, A&E nurses, health visitors, peer supporters and breastfeeding counsellors all attended the same sessions. Through these, they were able to understand each other’s roles and responsibilities and plan care together.
Peer supporters helped to run daily community drop-in groups with health visitors, and some worked in the antenatal clinic and postnatal wards of the hospital. Specialist, targeted peer support was offered to teenage parents, those with multiples and Somali mothers. A copy of Best Beginning’s ‘Bump to Breastfeeding’ DVD was given to all antenatal parents, who were also invited to a popular Saturday morning breastfeeding workshop.
Over a period of ten years, mothers felt comfortable breastfeeding their babies all over the borough and became visible in shopping centres, cafes, supermarkets, parks, and school grounds.
The National Maternity Review reported in 2016:
‘In Harrow, a multi-ethnic London borough with high infant mortality rates, and areas of deprivation and poverty, the Director of Public Health identified breastfeeding as a top priority for 2006. A multi-professional approach was adopted with Harrow Community Health Services working with the local hospital to improve breastfeeding rates. UNICEF Baby Friendly training was commissioned for midwives, health visitors and support staff in 2007. A peer support training programme began and mothers were recruited from a local support group. A network of breastfeeding support groups was established running from children’s centres, eventually achieving one every day within walking distance for all mothers. In 2008, Bump to Breastfeeding DVDs were given to every pregnant woman by midwives, health visitors and peer supporters. Harrow became accredited as Baby Friendly in 2012 and the local hospital gained the award in 2013. The staff training, peer support programme and free DVDs increased breastfeeding rates, so by 2010 initiation rates had risen to 82% and 6-8 weeks to 73%. By 2013, Harrow had 87% of mothers initiating and 75% breastfeeding at 6-8 weeks (50% exclusively), with one of the lowest drop-off rates in the UK. UNICEF assessed Harrow for its re-accreditation in 2014 and stated that it was the only local authority in the UK where breastfeeding was the ‘normal’ way to feed babies’.[1]
Other examples of Integrated community breastfeeding support:
This is the start of World Breastfeeding Week, which runs from the 1st to the 7th August each year. Our focus this year for Day 1 is Health Professionals.
“It takes a village to raise a child; it takes a community to support mothers to breastfeed
Sue Ashmore, Unicef UK Baby Friendly Initiative
Sue Ashmore of the Unicef UK Baby Friendly Initiative (BFI) wrote in 2017 ‘Just as the saying goes: ‘It takes a village to raise a child’, it takes a community to support mothers to breastfeed.’ (blog for the Huffington Post). That community includes health professionals but also breastfeeding specialists, such as IBCLCs and breastfeeding counsellors, and trained peer supporters.
Health professionals who have contact with mothers and their babies are a crucial part of that village of support. Since the WBTi report was pubished in 2016, an improvement has been the requirement of the NHS England Long-Term Plan (p.49) that all maternity units work towards achieving Baby Friendly accreditation. In comparison, all Scotland and N.I. maternity units were already accredited by 2016. Meeting this requirement will help provide a good basic standard of infant feeding support in English maternity units but as yet there is no requirement for neonatal units or community services (primarily that means the health visiting service) to achieve Baby Friendly status.
Summary table mapping UK health professional standards against WHO Educational Checklist on Infant and Young Child Feeding. See our report part 1 (for the table) and Part 2 (for details of individual health professions) https://ukbreastfeeding.org/wbtiuk2016/
The 2016 WBTi report highlighted the need for better training for most health professionals who work with new mothers. Since then, we’re very pleased to report that many more resources have been made available, including:
The GP Infant Feeding Network (GPIFN) and Hospital Infant Feeding Network (HIFN) were created and both have highly informative websites.
There have been some improvements to the paediatric and GP education curricula.
BFI has produced learning outcomes for students of several professions – medical, dietetic, pharmacy and maternity support workers/nursery nurses.
The University of Glasgow, working with BFI, has developed an e-learning module for first year medical students to support meeting the learning outcomes.
The Royal College of Paediatrics and Child Health has regularly updated its position statement on breastfeeding, the latest being June 2021, and includes: ‘RCPCH strongly supports breastfeeding, the promotion of breastfeeding, the provision of advice and support for women, and national policies, practices and legislation that are conducive to breastfeeding. All child health professionals should be trained to deliver simple breastfeeding advice.’
The Royal College of General Practitioners launched its position statement on breastfeeding in 2017 and then a free e-learning course on breastfeeding in 2018.
Thus some progress has been made towards the vision of all mothers who want to breastfeed being able to access seamless support from health professionals, additional breastfeeding specialists and trained peer supporters, all of whom value breastfeeding and are knowledgeable enough either to provide evidence-based information and support themselves or signpost to appropriate support.
A new study by trainee doctor Kirsty Biggs and senior colleagues has shown that 97% of the 411 medical students who responded to a survey are uncertain of their practical skills to support new mothers with breastfeeding, such as helping with latch issues, although the overall benefits of breastfeeding were moderately well-known. Yet most students (93%) perceived doctors to have an important role in supporting breastfeeding and the same percentage requested further breastfeeding education.
Over 80% of the respondents had a career interest in obstetric and gynaecology, paediatrics and/or general. While the sample was only around 1% of UK medical students, and only one-quarter of the students responding were male, it’s a very clear message that breastfeeding education overall is not adequate.
Around 80% of the 32 UK medical schools eligible responded to their part of the survey and results indicate that only 70% of medical schools provide compulsory breastfeeding education.
WBTI’s findings and vision
The WBTi UK report in 2016 indicated that medical curricula have many gaps with regard to breastfeeding, and Biggs’ study confirms that the students themselves find it inadequate. WBTi UK’s vision is that all doctors have sufficient training in infant feeding to protect the decisions of mothers who want to breastfeed.
How can the situation be improved? High level standards and Unicef BFI learning outcomes
The General Medical Council provides broad guidelines for undergraduate curricula in its Outcomes for Graduates document and each medical school devises its own curriculum to fit the guidelines. For example, the expectation under the Outcomes Health promotion and illness prevention section is: ‘Newly qualified doctors must be able to apply the principles, methods and knowledge of population health and the improvement of health and sustainable healthcare to medical practice’. Unicef UK Baby Friendly Initiative’s learning outcomes for several professions, including medical students, published in November 2019 are highly relevant to improving curricula and accompanying resources are being developed.
RCPCH curriculum – an encouraging sign
Medical training is long, with undergraduate, Foundation and then specialty training. The RCPCH (Royal College of Paediatrics and Child Health) states as part of its activity to promote breastfeeding: ‘The RCPCH training curriculum for General Paediatricians and all paediatric subspecialties requires training to understand the importance of breastfeeding and lactation physiology, be able to recognise common breastfeeding problems, have knowledge of formula and complementary feeding, and be able to advise mothers or refer for support.’
Mentioning infant feeding in guidance to doctors to encourage including it in consultations is also important. GP Louise Santhanam (founder of GPIFN) is the lead author of Postnatal Maternal and Infant careduring the COVID-19 Pandemic: a Guide for General Practicethat was recently added to the RCGP website. This clarifies that 6-8 week checks need to continue despite the Covid-19 pandemic and that infant feeding should be a routine clinical consideration.
Thus plenty of resources are available but doctors are busy people. While some really understand the importance of protecting breastfeeding, and know how to – such as signposting mothers to local skilled help – the challenge is how to bring this into every medical student’s training.
If you know anyone at medical school, it would be really useful if you can let them know about Kirsty Biggs’ study.
The Covid-19 pandemic has shown how important it is for countries to protect their citizens from illness.
Yet a new WBTi regional report shows gaps in support for families across Europe, with the poorest overall scores in national leadership and, shockingly, emergency preparedness, where the UK scored 0/10. This pandemic is an emergency for infants and young children and only North Macedonia was found to have an adequate strategy.
Babies who are breastfed have better health and resistance to infection, and most mothers want to breastfeed. Yet many European mothers stop or reduce breastfeeding in the early weeks and months, and bottle feeding is prevalent, due to inadequate support from health systems and society.
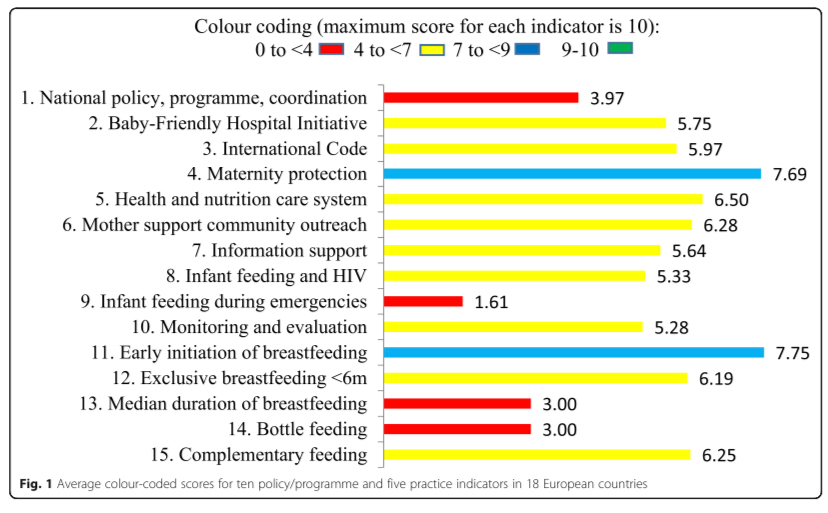
Launched today, the first European report on infant and young child feeding policies and practices, Are our babies off to a healthy start?, compares 18 countries and identifies the considerable improvements they need to make in supporting mothers who want to breastfeed. A summary report has been published today in theInternational Breastfeeding Journal.
The new report, Are our babies off to a healthy start?, compares the implementation of WHO’s Global Strategy for Infant and Young Child Feeding across 18 European countries. The comparisons show clearly that inadequate support and protection for breastfeeding mothers is a Europe-wide problem. The health of babies, mothers and whole populations lose out as a result. However, countries do differ considerably. Turkey rates highest overall; the five countries with the lowest scores belong to the European Union.
‘Nutrition is key to achieving the Sustainable Development Goals related to health, education, sustainable development, reduction of inequalities and more.’
Joao Breda, Head, WHO European Office for Prevention and Control of Noncommunicable Diseases
The scope of the assessment is wide-ranging, with ten policy and programme indicators, including national leadership, Baby Friendly hospital and community practices, marketing controls on breastmilk substitutes, health professional training, emergency preparedness and monitoring. There are also five feeding practices indicators, such as exclusive breastfeeding for 6 months, a WHO recommendation.
The original assessments were all carried out using the World Breastfeeding Trends Initiative (WBTi), a tool first developed in 2004 by the International Baby Food Action Network (IBFAN) but only launched in Europe in 2015. It requires collaboration with relevant organisations within a country on assessment scores, gaps identified and recommendations for improvements. The Report highlights good practice, enabling countries to learn from one another.
˝Success …rests first and foremost on achieving political commitment at the highest level and assembling the indispensable human and financial resources.’
WHO Global Strategy 2003
If governments, other policymakers, hospitals and community services, public health departments, institutions that train health professionals, and others, adopt the report recommendations, it will enable more mothers to initiate and continue breastfeeding, strengthening the health of the population for the future.
The WBTi European Working Group, led by Dr. Irena Zakarija-Grkovic of Croatia, produced the Report and comprises coordinators from European countries which have carried out a WBTi assessment. The production of the report was supported by the Croatian Ministry of Health and UNICEF Croatia.
2016 WBTi Report on the UK : see Indicator 5 for health professional training, with the main summary table in Part 1 and details for individual professions in Part 2.
Working with public services to support families better with infant feeding and developing close loving relationships through training and accreditation
Doctors have an important role to play in supporting mothers who want to breastfeed.
A continuing theme of the WBTi UK work is improving medical training in infant feeding such that all, not just some, doctors have sufficient knowledge and understanding of breastfeeding to protect the decisions of mothers who want to breastfeed. Enabling more mothers to continue breastfeeding would improve infant and maternal health, reduce NHS costs (Renfrew et al) and reduce the number of GP appointments (Pokhrel et al, 2015).
Supporting Mothers Who Breastfeed, by Patricia Wise. E-book downloadable from the WBTI website
Georgie BHS and Dani Phillipson from the Parenting Science Gang, which runs citizens’ science projects using mothers to collect evidence, spoke next. They described the breastfeeding and healthcare experiences project (inspired in part by the WBTi findings on health professional training) with its subsidiary small project of 8 interviews looking at healthcare professionals’ own experiences of breastfeeding on their professional practice. From the themes identified, PSG has produced MILK cards to guide health professionals:
Mothers’ voices matter
Investigate common issues, but also
Look for underlying causes§
Know where to find information
GP Dr. Terri Lovis (seen in banner photo above) described how the GP Infant Feeding Network (GPIFN), initiated by Dr. Louise Santhanam, was set up as a pharma free network to improve the quality of support in infant feeding with the work provided voluntarily. The website is a comprehensive educational resource for primary care and there is partnership with the Hospital Infant Feeding Network (HIFN). Additional achievements include working collaboratively with IMAP (International Milk Allergy in Primary Care Guidelines) to produce the 2019 version and bidding successfully with PHE and Surrey Heartlands to train Infant Feeding champions across Surrey (as Norwich already does).
Dr Natalie Shenker from the Human Milk Foundation
The fascinating keynote presentation was by Dr. Natalie Shenker on Doctors and Breastmilk, and included the initiation of the Human Milk Foundation in 2017 and the work of the Hearts Milk Bank, which she co-founded with Gillian Weaver. The Milk Bank is involved in research as well as providing pasteurised donor milk.
The challenge is how to enable all medical students, trainees and qualified doctors to acquire an adequate minimum standard in infant feeding knowledge and skills. Yes, there is a huge amount that they need to know in total but being breastfed as an infant can make such a difference to the health of baby and mother (not to mention the environmental sustainability of breastfeeding!) that it is crucial to include. Some examples of what is already being done to help achieve this:
Imperial College Medical School is running a programme in which medical students are allocated to follow a mother from the end of pregnancy until the child is 3 years old.
Norwich CCG has a GP Champion in Infant Feeding scheme, which Surrey Heartlands is also rolling out, in which the champion receives training and disseminates the learning throughout the practice.
Imagine if all medical schools ran such a programme and all GP practices had a breastfeeding champion!
Banner photo: Dr. Terri Lovis
Patricia Wise is the author of ‘Supporting Mothers Who Breastfeed: A Guide for Trainee and Qualified Doctors’. She is an NCT Breastfeeding Counsellor and tutor, and a member of the WBTi UK Steering Group
The WBTi UK team are proud to be part of producing this joint statement calling for our next government to make breastfeeding a priority in setting the agenda to prioritise the early years of life.
The new government needs to prioritise the first 1001 days of a child’s life, from conception to age two, to enable children to survive and thrive. How an infant is fed and nurtured strongly influences a child’s future life chances and emotional health. Importantly, if a woman breastfeeds there are substantial health benefits for her – having impacts onher future long after breastfeeding has stopped.
Independent, practical, evidence-based information and support is essential for every family. Supporting women with breastfeeding can go a long way to protecting children and mothers from a wide range of preventable ill health, including obesity and mental health problems.
This window of opportunity cannot be missed for the future health outcomes of mothers and the next generation. In addition to well documented health outcomes, supporting breastfeeding will also contribute to a stronger economy – potential annual savings to the NHS are estimated at about £40 million per year from just a moderate increase in breastfeeding rates.
Support for breastfeeding is also an environmental imperative and recognition of the contribution breastfeeding can make to avoiding environmental degradation should be a matter of increasing global and political attention.
In the UK, the majority of women start to breastfeed but breastfeeding rates drop rapidly – our continuation rates are some of the lowest in the world and are even lower amongst women living in deprived areas, where increasing rates could make a real difference to health inequalities. Support for all women, parents and families with breastfeeding falls short of what is wanted and needed.
Women tell us they encounter difficulties with the public perceptions of breastfeeding out of the home. Families tell us they are still regularly exposed to conflicting messaging and marketing for formula milks that drowns out advice from healthcare professionals.
Women tell us they receive little to no help with infant feeding and that their health visitors, midwives and doctors often have little training or knowledge about breastfeeding and limited time to support them.
Recent cuts in health visitor numbers and breastfeeding peer support services mean many women may be left without the support they need however they choose to feed their infants.
Despite robust evidence showing that investment in breastfeeding support and protection makes sense, politically breastfeeding has been viewed by governments as a lifestyle choice and so left to parents to work out for themselves. For too many women, trying to breastfeed without support, or stopping before they want to, is deeply upsetting and the situation is made worse by fragmented care, and poor and often conflicting advice from those they are seeking to support them. To ensure an increase in breastfeeding rates, to help reverse obesity rates and to reduce widening health inequalities will require significant investment in breastfeeding.
It is essential that our new government prioritises breastfeeding and invests in its support and protection.
We call on all political parties to commit to the following actions, if elected:
To appoint a permanent, multi-sectoral infant and young child feeding strategy group and develop, fund and implement a national strategy to improve infant and young child feeding practices.
To include actions to promote, protect and support breastfeeding in all policy areas where breastfeeding has an impact.
To implement the Unicef UK Baby Friendly Initiative across community and paediatric services, building on the recommendation for maternity services in the NHS Long Term Plan.
To protect babies from harmful commercial interests by bringing the full International Code of Marketing of Breastmilk Substitutes into UK law and enforcing this law.
To commission, and sustainably fund, universal breastfeeding support programmes delivered by specialist/lead midwives and health visitors or suitably qualified breastfeeding specialists, such as IBCLC lactation consultants and breastfeeding counsellors, alongside trained peer supporters with accredited qualifications.
To maintain and expand universal, accessible, affordable and confidential breastfeeding support through the National Breastfeeding Helpline and sustaining the Drugs in Breastmilk Service.
To deliver universal health visiting services and the Healthy Child Programme by linking in with local specialist and support services.
To establish/re-establish universal Children’s Centres with a focus on areas of deprivation, offering breastfeeding peer support.
To make it a statutory right of working mothers and those in education to work flexibly as required and to access a private space and paid breaks to breastfeed and/or express breastmilk and manage its safe storage.
To commit to resourcing for charitableorganisations who play a key role within the health agenda working at a national and local level to support families and communities with infant feeding.
To support the commitment to undertake an Infant Feeding Survey which builds on the data previously collected in the Infant Feeding Survey 2010 (now discontinued).
To implement the recommendations of the Becoming Breastfeeding Friendly (BBF) study.
CASE FOR ACTION
Breastfeeding benefits all babies, and studies have shown that just a small increase in breastfeeding rates could cut NHS expenditure considerably. It is vital to invest in breastfeeding support in the early months and this will reap rewards in the future that are likely to exceed the initial cash flows associated with putting proper support in place.
A UNICEF reportstates that “no other health behaviour has such a broad-spectrum and long-lasting impact on public health. The good foundations and strong emotional bonds provided in the early postnatal period and through breastfeeding can affect a child’s subsequent life chances”.
Evidence has also demonstrated that a child from a low-income background who is breastfed is likely to have better health outcomes than a child from a more affluent background who is formula-fed. Breastfeeding provides one solution to the long-standing problem of health inequality.
Research into the extent of the burden of disease associated with low breastfeeding rates is hampered by data collection methods. This can be addressed by investment in good quality research.
2. Borra C, Iacovou M, Sevilla A (2015) Maternal Child Health Journal (4): 897-907. New evidence on breastfeeding and postpartum depression: the importance of understanding women’s intentions.
3. Brown, A, Rance J, Bennett, P (2015) Understanding the relationship between breastfeeding and postnatal depression: the role of pain and physical difficulties. Journal of Advanced Nursing72 (2): 273-282
10. National Institute for Health and Care Excellence (2012) Improved access to peersupport NICE, London
11. Rollins N, Bhandari N, Hajeebhoy N, et al (2016) Why invest, and what it will take to improve breastfeeding practices? The Lancet387 491-504
12. Wilson AC, Forsyth JS, Greene SA, Irvine L, Hau C, Howie PW. 1998 Relation of infant diet to childhood health: seven year follow up of cohort of children in Dundee infant feeding study. BMJ. Jan 3;316(7124):21-5.