WHO and UNICEF launched the Baby Friendly Initiative (BFHI) over thirty years ago; three years later, UNICEF UK Baby Friendly Initiative (BFI) was born. The original BFHI framework of Ten Steps was created to improve maternity and hospital practices that undermined breastfeeding, such as separating mothers and their newborns or routine formula supplements, as well as implementing the International Code of Breastmilk Substitutes in maternity settings, in order to eliminate conflicts of interest with the baby feeding industry (companies that manufacture or distribute infant formula/milks, baby foods, feeding bottles and teats) such as promotion of formula milk in healthcare settings, or direct contact by companies with parents.
The Baby Friendly Initiative has changed the face of maternity practices and midwifery training in the UK – breastfeeding initiation has gone up about 20% since UNICEF UK BFI was founded in 1994. In this country, BFI has grown beyond maternity settings to create standards for infant feeding support programmes in the community and for universities training the next generation of midwives and health visitors.The BFI standards were revised in 2012, based upon the twin pillars of breastfeeding and the UN Convention on the Rights of the Child.
Routine care: all staff in the universal services (midwives, health visitors, support workers etc) are trained to BFI standard with sound, evidence-based, basic training in supporting breastfeeding and responsive infant feeding.
Additional services: every area should have additional support available, such as trained, skilled peer supporters who can act as an “informed friend” for new mothers, and a network of local peer support groups where new parents can find social support alongside help with everyday breastfeeding issues.
Specialist services: every area should also have a referral pathway for specialist care for more complex breastfeeding problems; breastfeeding specialists should have extensive experience or training such as the IBCLC qualification or a recognised breastfeeding counsellor/supporter credential, and either be a registered health professional themselves, or co-lead the specialist service with a registered health professional.
WBTi poster on Integrated Services to Support Breastfeeding, 2019
A good example of how the BFI community standards work is Harrow. Read more HERE about how WBTi UK Steering Team member and specialist health visitor Alison Spiro led Harrow’s local community health services through BFI accreditation, to develop a well integrated services and become
“the only local authority in the UK where breastfeeding was the ‘normal’ way to feed babies”
More recently, UNICEF UK BFI have produced Learning Outcomes for a wider range of health professions: medical students, paediatricians, pharmacists, paediatric/ children’s nurses, maternity support workers and nursery nurses. These will help to address the gaps in high level health professional training standards found in WBTI’s 2016 report. Every health professional who works with women, infants and children should understand the basics of lactation and breastfeeding management, prescribing during lactation, and how to refer parents on to local breastfeeding support.
#WBW2022 Webinar
On Wednesday 3 August, we will all have the chance to learn more about the Ten Steps of BFHI in a webinar produced by the Global Breastfeeding Collective, an alliance of NGOs from around the world led by WHO and UNICEF.
In addition, there will be sessions on the care of young breastfed infants who are small or with faltering growth (the MAMI Pathway) and on infant feeding in emergencies.
The entire webinar runs from 7-9 AM BST and again from 4-6 PM BST, and will be recorded.
It takes a village to raise a child – we all have a role to play to support breastfeeding mothers and babies.
We all are the building blocks responsible for supporting new families: partners and family members, health workers, neighbours and community members, religious leaders, employers, academics, governments and policy makers. We can all make a difference. We need to step up to our responsibilities. Everyone needs to understand the importance of breastfeeding – for maternal and infant physical and mental health and wellbeing, for public health, for our economy, and for our planet.
For WBW this year, WABA has produced an extensive suite of materials looking at all these roles and responsibilities. They have outlined the challenges that breastfeeding families face at every stage from conception, through birth, getting breastfeeding off to a good start, and maintaining breastfeeding all the way through starting solids and going back to work, and the solutions we need in each situation – all backed up by links to the latest evidence.
The #WBW2022 Action Folder pulls all this together: it is a useful resource for anyone using evidence to build policies and best practice. You can download it as a PDF and all the links to research and references will be live.
The UK WBTi team will be highlighting just a few of the concepts this week:
Health workers: the importance of relevant, evidence-based. The advertising of follow-on milks, on the media, from 6 months in the UK has led to confusion, resulting in some parents seeing formula milk as equivalent to breastmilk, or that breastfeeding should stop at 6 months. The International Code needs to be adopted by the UK government in full, to reduce this confusion and protect breastfeeding. training for all those who work with women, infants and young children
UNICEF UK Baby Friendly Initiative and the BFHI worldwide sets out ways in which healthcare staff can receive sound, evidence-based, basic training in supporting breastfeeding.
ALSO join a special webinar from the Global Breastfeeding Collective on BFHI, with some added specialist topics on supporting small and underweight breastfeeding infants, and on infant feeding in emergencies. (7-9 AM BST and again at 4-6 PM BST). Register HERE
Community support: Access to skilled, integrated support for all, with a special focus in the GBC webinar on how to support breastfeeding infants who are not gaining well (NICE NG 75,2017). All parents should have easy access to trained healthcare staff- midwives, paediatricians, health visitors and GPs- breastfeeding peer supporters and specialist support (IBCLC, BFCs). Supporting breastfeeding in complex circumstances: Specialist support from IBCLCS, BFCs, or infant feeding leads, integrated with specialist healthcare teams
Protecting infants and young children in emergencies. National policies should guide Local Resilience Forums but these do not exist at present.
The impact of misleading marketing: The International Code. The advertising of follow-on milks, on the media, from 6 months in the UK has led to confusion, resulting in some parents seeing formula milk as equivalent to breastmilk, or that breastfeeding should stop at 6 months. The International Code needs to be adopted by the UK government in full, to reduce this confusion and protect breastfeeding.
Governments with national and local policy makers need to protect all families and support them to make informed feeding decisions free of commercial influence.
What can YOU do?
It is time for a reassessment of the UK’s national infant feeding policies and programmes. YOU could help! Volunteers are welcome with knowledge in any of the ten policy areas (Indicators 1-10), or with skills such as research, writing, graphics, social media and more – feel free to contact us for a chat!
WBTi Key Indicators:
Indicator 1: National policy, programme and coordination Indicator 2: Baby Friendly Initiative Indicator 3: International Code of Marketing of Breastmilk Substitutes
Indicator 4: Maternity protection Indicator 5: Health professional training Indicator 6: Community-based support Indicator 7: Information support Indicator 8: Infant feeding and HIV
Indicator 9: Infant and young child feeding during emergencies
Indicator 10: Monitoring and evaluation
Which one will YOU choose?
Contact us: wbti@ukbreastfeeding.org
Helen Gray MPhil IBCLC is Joint Coordinator of the WBTi UK Steering Group.
The Covid-19 pandemic has shown how important it is for countries to protect their citizens from illness.
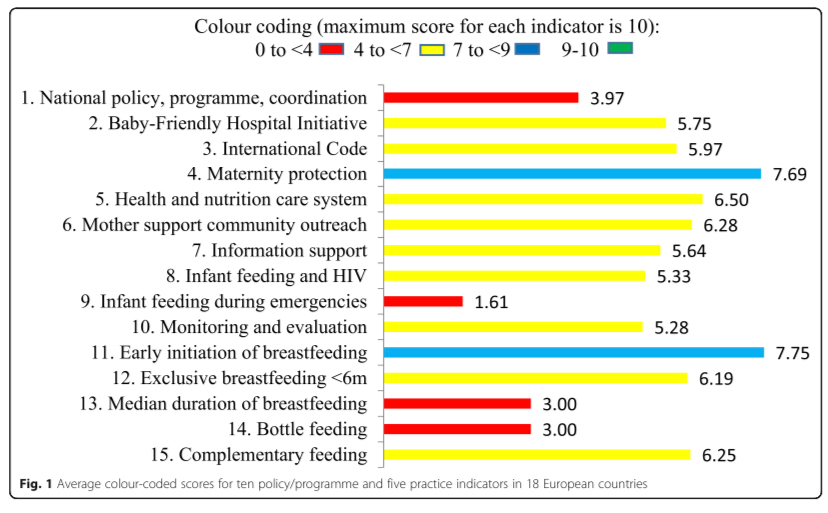
Yet a new WBTi regional report shows gaps in support for families across Europe, with the poorest overall scores in national leadership and, shockingly, emergency preparedness, where the UK scored 0/10. This pandemic is an emergency for infants and young children and only North Macedonia was found to have an adequate strategy.
Babies who are breastfed have better health and resistance to infection, and most mothers want to breastfeed. Yet many European mothers stop or reduce breastfeeding in the early weeks and months, and bottle feeding is prevalent, due to inadequate support from health systems and society.
Launched today, the first European report on infant and young child feeding policies and practices, Are our babies off to a healthy start?, compares 18 countries and identifies the considerable improvements they need to make in supporting mothers who want to breastfeed. A summary report has been published today in theInternational Breastfeeding Journal.
The new report, Are our babies off to a healthy start?, compares the implementation of WHO’s Global Strategy for Infant and Young Child Feeding across 18 European countries. The comparisons show clearly that inadequate support and protection for breastfeeding mothers is a Europe-wide problem. The health of babies, mothers and whole populations lose out as a result. However, countries do differ considerably. Turkey rates highest overall; the five countries with the lowest scores belong to the European Union.
‘Nutrition is key to achieving the Sustainable Development Goals related to health, education, sustainable development, reduction of inequalities and more.’
Joao Breda, Head, WHO European Office for Prevention and Control of Noncommunicable Diseases
The scope of the assessment is wide-ranging, with ten policy and programme indicators, including national leadership, Baby Friendly hospital and community practices, marketing controls on breastmilk substitutes, health professional training, emergency preparedness and monitoring. There are also five feeding practices indicators, such as exclusive breastfeeding for 6 months, a WHO recommendation.
The original assessments were all carried out using the World Breastfeeding Trends Initiative (WBTi), a tool first developed in 2004 by the International Baby Food Action Network (IBFAN) but only launched in Europe in 2015. It requires collaboration with relevant organisations within a country on assessment scores, gaps identified and recommendations for improvements. The Report highlights good practice, enabling countries to learn from one another.
˝Success …rests first and foremost on achieving political commitment at the highest level and assembling the indispensable human and financial resources.’
WHO Global Strategy 2003
If governments, other policymakers, hospitals and community services, public health departments, institutions that train health professionals, and others, adopt the report recommendations, it will enable more mothers to initiate and continue breastfeeding, strengthening the health of the population for the future.
The WBTi European Working Group, led by Dr. Irena Zakarija-Grkovic of Croatia, produced the Report and comprises coordinators from European countries which have carried out a WBTi assessment. The production of the report was supported by the Croatian Ministry of Health and UNICEF Croatia.
The WBTi UK team are proud to be part of producing this joint statement calling for our next government to make breastfeeding a priority in setting the agenda to prioritise the early years of life.
The new government needs to prioritise the first 1001 days of a child’s life, from conception to age two, to enable children to survive and thrive. How an infant is fed and nurtured strongly influences a child’s future life chances and emotional health. Importantly, if a woman breastfeeds there are substantial health benefits for her – having impacts onher future long after breastfeeding has stopped.
Independent, practical, evidence-based information and support is essential for every family. Supporting women with breastfeeding can go a long way to protecting children and mothers from a wide range of preventable ill health, including obesity and mental health problems.
This window of opportunity cannot be missed for the future health outcomes of mothers and the next generation. In addition to well documented health outcomes, supporting breastfeeding will also contribute to a stronger economy – potential annual savings to the NHS are estimated at about £40 million per year from just a moderate increase in breastfeeding rates.
Support for breastfeeding is also an environmental imperative and recognition of the contribution breastfeeding can make to avoiding environmental degradation should be a matter of increasing global and political attention.
In the UK, the majority of women start to breastfeed but breastfeeding rates drop rapidly – our continuation rates are some of the lowest in the world and are even lower amongst women living in deprived areas, where increasing rates could make a real difference to health inequalities. Support for all women, parents and families with breastfeeding falls short of what is wanted and needed.
Women tell us they encounter difficulties with the public perceptions of breastfeeding out of the home. Families tell us they are still regularly exposed to conflicting messaging and marketing for formula milks that drowns out advice from healthcare professionals.
Women tell us they receive little to no help with infant feeding and that their health visitors, midwives and doctors often have little training or knowledge about breastfeeding and limited time to support them.
Recent cuts in health visitor numbers and breastfeeding peer support services mean many women may be left without the support they need however they choose to feed their infants.
Despite robust evidence showing that investment in breastfeeding support and protection makes sense, politically breastfeeding has been viewed by governments as a lifestyle choice and so left to parents to work out for themselves. For too many women, trying to breastfeed without support, or stopping before they want to, is deeply upsetting and the situation is made worse by fragmented care, and poor and often conflicting advice from those they are seeking to support them. To ensure an increase in breastfeeding rates, to help reverse obesity rates and to reduce widening health inequalities will require significant investment in breastfeeding.
It is essential that our new government prioritises breastfeeding and invests in its support and protection.
We call on all political parties to commit to the following actions, if elected:
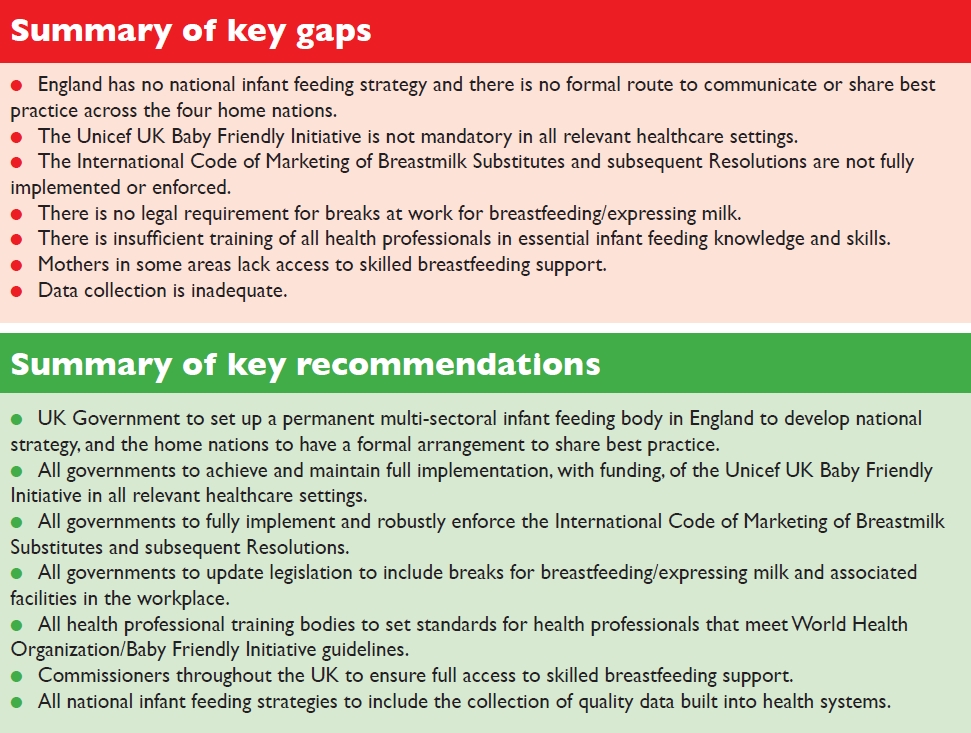
To appoint a permanent, multi-sectoral infant and young child feeding strategy group and develop, fund and implement a national strategy to improve infant and young child feeding practices.
To include actions to promote, protect and support breastfeeding in all policy areas where breastfeeding has an impact.
To implement the Unicef UK Baby Friendly Initiative across community and paediatric services, building on the recommendation for maternity services in the NHS Long Term Plan.
To protect babies from harmful commercial interests by bringing the full International Code of Marketing of Breastmilk Substitutes into UK law and enforcing this law.
To commission, and sustainably fund, universal breastfeeding support programmes delivered by specialist/lead midwives and health visitors or suitably qualified breastfeeding specialists, such as IBCLC lactation consultants and breastfeeding counsellors, alongside trained peer supporters with accredited qualifications.
To maintain and expand universal, accessible, affordable and confidential breastfeeding support through the National Breastfeeding Helpline and sustaining the Drugs in Breastmilk Service.
To deliver universal health visiting services and the Healthy Child Programme by linking in with local specialist and support services.
To establish/re-establish universal Children’s Centres with a focus on areas of deprivation, offering breastfeeding peer support.
To make it a statutory right of working mothers and those in education to work flexibly as required and to access a private space and paid breaks to breastfeed and/or express breastmilk and manage its safe storage.
To commit to resourcing for charitableorganisations who play a key role within the health agenda working at a national and local level to support families and communities with infant feeding.
To support the commitment to undertake an Infant Feeding Survey which builds on the data previously collected in the Infant Feeding Survey 2010 (now discontinued).
To implement the recommendations of the Becoming Breastfeeding Friendly (BBF) study.
CASE FOR ACTION
Breastfeeding benefits all babies, and studies have shown that just a small increase in breastfeeding rates could cut NHS expenditure considerably. It is vital to invest in breastfeeding support in the early months and this will reap rewards in the future that are likely to exceed the initial cash flows associated with putting proper support in place.
A UNICEF reportstates that “no other health behaviour has such a broad-spectrum and long-lasting impact on public health. The good foundations and strong emotional bonds provided in the early postnatal period and through breastfeeding can affect a child’s subsequent life chances”.
Evidence has also demonstrated that a child from a low-income background who is breastfed is likely to have better health outcomes than a child from a more affluent background who is formula-fed. Breastfeeding provides one solution to the long-standing problem of health inequality.
Research into the extent of the burden of disease associated with low breastfeeding rates is hampered by data collection methods. This can be addressed by investment in good quality research.
2. Borra C, Iacovou M, Sevilla A (2015) Maternal Child Health Journal (4): 897-907. New evidence on breastfeeding and postpartum depression: the importance of understanding women’s intentions.
3. Brown, A, Rance J, Bennett, P (2015) Understanding the relationship between breastfeeding and postnatal depression: the role of pain and physical difficulties. Journal of Advanced Nursing72 (2): 273-282
10. National Institute for Health and Care Excellence (2012) Improved access to peersupport NICE, London
11. Rollins N, Bhandari N, Hajeebhoy N, et al (2016) Why invest, and what it will take to improve breastfeeding practices? The Lancet387 491-504
12. Wilson AC, Forsyth JS, Greene SA, Irvine L, Hau C, Howie PW. 1998 Relation of infant diet to childhood health: seven year follow up of cohort of children in Dundee infant feeding study. BMJ. Jan 3;316(7124):21-5.
The theme for World Breastfeeding Week this year is “Empower parents, enable breastfeeding,” which fits the philosophy of our WBTi work very well. The WBTi recommendations have been produced by a Core Group of 18 of the UK’s key government agencies, health professional organisations and charities working in infant and maternal health. The 46 recommendations, across ten areas of policy and programmes, parallel many of the recommendations of previous national breastfeeding initiatives such as the UNICEF Baby Friendly Call to Action, the Becoming Breastfeeding Friendly project (completed in Wales and Scotland so far), and the Breastfeeding Manifesto.
The WBTi assessment and recommendations for action are all about providing the structures, policies and programmes that families need in order to support mothers and infants to be able to breastfeed successfully. It is not a woman’s responsibility on her own, it is the responsibility of ALL of us, across society, to provide the support that mothers and babies need.
Our UK report found many gaps and barriers in ten areas of policy and programmes across the UK:
Lack of national leadership and national strategy on infant feeding, except in Scotland.
Areas where maternity settings still do not meet the minimum UNICEF Baby Friendly standards, in particular in England.
Weak regulations governing marketing by baby milk companies, no regulations governing bottle and teat marketing, and little enforcement of existing provisions.
Lack of provisions to support new mothers to continue breastfeeding when they return to work.
Gaps in health care professional training in infant and young child feeding (See both Part 1 and Part 2 of the WBTi report for full details)
Cuts to peer support and other community breastfeeding support.
No national communications strategy on breastfeeding.
Lack of understanding of current guidance on breastfeeding for HIV+ mothers.
No national guidance on planning for the care of infants and young children in emergencies or disasters.
Poor data collection and monitoring of breastfeeding rates.
Highlights of progress
There are several bright spots, however, and in the two years since the WBTi report and recommendations were published, there have been improvements in several areas
National policy work: Scotland already had strong national policy leadership. Scotland, Wales and England have taken part in the Becoming Breastfeeding Friendly project on scaling up breastfeeding interventions, with a government commitment to act on recommendations.
With the latest NHS England Long Term Plan, all of the UK has now pledged to reach full UNICEF Baby Friendly accreditation in all maternity settings.
Increased awareness of International Code issues in the UK include a relaunch of the UK Baby Feeding Law Group, a coalition of UK organisations working in infant and maternal health, to advocate for implementation of the International Code in UK law.
The Alliance for Maternity Rights has included the protection of flexible breastfeeding/ expressing breaks and suitable facilities in their Action Plan.
Several health professional councils have begun to review their training standards on infant feeding, and a working group led be UNICEF Baby Friendly has launched a new set of learning outcomes for the training of medical students, paediatric nurses, dietitians, pharmacists and maternity support workers/ nursery nurses.
Continued cuts to local authority and public health budgets has continued to severely impact community breastfeeding support such as trained peer support. The WBTi team organised a conference on the public health impact of breastfeeding with the Institute for Health Visiting, exploring in particular the UNICEF Baby Friendly community requirements for “basic” health professional BFI training, “additional” local trained support such as peer support groups, and a “specialist” referral pathway at IBCLC level. The BFI, NICE and Public Health England guidance are clearly explained in the “Guide to the Guidance” by Better Breastfeeding. However there is potential for strengthening the commissioning of integrated breastfeeding services, through the increased profile of breastfeeding in England in the NHS Long Term Plan, breastfeeding representation now being included in the NHS England National Maternity Transformation Programme Stakeholder Group, and in Scotland and Wales with renewed national leadership and funding.
Although no national communication strategies on breastfeeding have been developed, the national governments and public health agencies have developed breastfeeding campaigns and have supported national breastfeeding weeks again across all four nations.
Infant feeding in emergencies is still not covered by national guidance or universally in local disaster resilience planning, however a national forum hosted by Alison Thewliss MP, and led by the UK WBTI team and Dr Ruth Stirton from the University of Sussex Law School has kick-started the discussion to improve awareness and standards.
So we are in interesting times – we still face budgetary and cultural challenges, and families still face many barriers.
However change is clearly happening!
Coming up on the WBTi blog for #WBW2019
For World Breastfeeding Week, we are hosting a number of guest blogs detailing some exciting innovations: The launch of the Hospital Infant Feeding Network, with a website and a collection of posters and resources for health professionals working with mothers, infants and young children in hospital.
A new set of educational resources on breastfeeding and medications for pharmacists, from the wonderful Wendy Jones.
And a blog looking at some of the public health issues around breastfeeding support in the community, from Alice Allan IBCLC MPH.
Sign up HERE for WBTi’s email list, and don’t forget to sign up to follow our blog!
Helen Gray IBCLC is Joint Coordinator of the WBTi UK team, with a special interest in supporting families in emergencies.
Just as a partridge can find support and protection in the branches of a pear tree, each breastfeeding dyad needs a society that provides a supportive structure; to achieve this needs coordination at national level through having a national policy, a strategic plan and effective implementation of that plan (WBTi Indicator 1).
Jeremy Hunt, when Secretary of State for Health, declared that
“The government is implementing the vision set out in the WBTi UK report. The Maternity Transformation Programme seeks to achieve the vision set out in the report by bringing together a wide range of organisations to work in nine areas… this includes promoting the benefits of breastfeeding by
Providing national leadership for breastfeeding celebration week;
Publishing breastfeeding initiation data;
Publishing breastfeeding profiles; and
Improving the quality of data on breastfeeding prevalence at 6-8 weeks after birth.”
A national assessment of UK breastfeeding policies and programmes, “Becoming Breastfeeding Friendly,” has now begun across England, Scotland, and Wales, led by the national governments and public health agencies and the University of Kent. Importantly, this initiative requires government commitment to implementing the resulting recommendations.
Another positive development since the WBTi report in 2016 is that in April 2018 Public Health England created a one-year Midwifery Adviser post for a seconded health professional whose responsibilities include breastfeeding, funded by the National Maternity Transformation Programme.
Day 2 – two turtle doves
This fits very well with Indicator 2 as it assesses the extent to which maternity-related services are Baby-Friendly accredited and the standards support loving relationships. Since the WBTi report, percentages of UK accreditations have increased as follows (2016 figure in brackets):
maternity services 62% (58%)
health visiting services 67% (62%)
universities: 43% (36%) midwifery and 17% (15%) of health visiting courses
childrens’ centres 16 (0)
neonatal units 6 (0)
Births taking place in fully accredited hospitals:
The WBTi recommendations call for “implementation and maintenance of Baby Friendly standards in all healthcare settings” in England and Wales. New maternity plans in December 2018 from the Department for Health and Social Care include “asking all maternity services to deliver an accredited, evidence-based infant feeding programme in 2019 to 2020, such as the UNICEF Baby Friendly initiative.” We would urge the government to extend the expectation of Unicef Baby Friendly accreditation as a minimum in community settings and Health Visiting Services, in neonatal units, and in midwifery and health visitor training programmes.
Day 3 – three French hens
The French hens are believed to symbolise the virtues of faith, hope and charity. Indicator 3 assesses the extent of implementation of the International Code of Marketing of Breastmilk Substitutes and subsequent WHA resolutions. There is faith, that incorporating the Code and resolutions in a country’s laws improves protection for all babies from commercial interests, as the experiences of individual countries like Brazil shows. There is hope that the Code and Resolutions will one day be implemented in UK law. Charity includes helping the vulnerable, such as babies.
Relatively recent changes include the World Health Assembly passing resolution 69.9 in May 2016, welcoming the new World Health Organisation 2016 guidance which clarifies that the Code applies to all milks and commercially produced foods marketed as suitable for infants and young children up to 36 months. A new Implementation Manual for this WHO guidance is also available.
In addition, the First Steps Nutrition Trust is now taking on the role of secretariat to the Baby Feeding Law Group (BFLG), a coalition of UK organisations working in maternal and infant health who work to bring UK law into compliance with the International Code. The WBTi UK Steering team is a member of the BFLG.
Day 4 – four calling birds
Indicator 4 assesses the protection and support provided by workplaces for employees who are breastfeeding. Four organisations helping to improve the situation include:
WBTi UK, which made several recommendations in its report, including that tribunal access is available to women in all income brackets.
Gold is associated with precious things, and colostrum is known as “liquid gold.”
Indicator 5 assesses both the extent to which care providers are trained in infant and young child feeding and how supportive health service policies are. There are five professions which work most closely with mothers, infants and young children: midwives, obstetricians, paediatricians, health visitors and GPs. If they value breastfeeding and have the training to support mothers effectively they can serve as a golden chain of support.
The midwifery standards are currently undergoing a thorough review and there will be a consultation in February 2019.
Members of the WBTi team have been supporting the work of revising and updating professional standards, and a working group led by Unicef Baby Friendly has now formed to take this work forward.
Day 6 – six geese a-laying
In the song the geese symbolise the six days of creation.
Indicator 6 covers community-based support. So many mothers stop breastfeeding before they want to that it is really important to create an integrated system of support to avoid mothers falling into gaps between services. Six key aspects are:
Basic support: Health visitors and other health workers trained to a minimum Baby Friendly standard provide basic but universal help with feeding.
Additional: A peer support programme with trained peer supporters provides ongoing social support.
Specialist: For more challenging situations, mothers need to be able to access specialist help, for example from certified lactation consultants and breastfeeding counsellors.
Matt Hancock, UK Secretary of State for Health and Social Care since July 2018, launched his prevention vision on 5 November.
His other priorities are to advance health technology and provide better support for the health and social care workforce. He sees prevention as having two aspects. Partly it is about keeping well physically and mentally, to prevent ill health, but also about the environment around people, their lifestyle choices and how existing health conditions are managed. The aims are for the average person to have 5 more years of healthy independent living by 2035, and to reduce the gap between the richest and poorest. At present there is a large discrepancy in spending with £97 billion (public money) spent on treating disease and £8 billion on prevention across the UK!
The proposed actions in the vision are:
“Prioritising investment in primary and community healthcare
Making sure every child has the best start in life (our emphasis)
Supporting local councils to take the lead in improving health locally through innovation, communication and community outreach
Coordinating transport, housing, education, the workplace and the environment – in the grand enterprise to improve our nation’s health
Involving employers, businesses, charities, the voluntary sector and local groups in creating safe, connected and healthy neighbourhoods and workplaces”
It states there is strong evidence that prevention works and recognises that a healthy population is both vital for a strong economy and for reducing pressure on services like the NHS (almost 10% of the national income is spent on healthcare). Average life expectancy is now 81 years, helped by:
advances in healthcare
changing attitudes so there is less stigma with some conditions
improvements in the environment, at home, work and in neighbourhoods
antibiotics and mass vaccination
public health programmes.
However, there are major challenges in the huge discrepancies between areas – ‘A boy born today in the most deprived area of England can expect to live about 19 fewer years in good health and die nine years earlier than a boy born into the least deprived area.’ (p.7)
Improvements will depend both on encouraging individuals to choose healthy lifestyles and manage their own health, and expecting local authorities to take the lead in improving the health of their communities. The challenges of smoking, mental ill health, obesity, high blood pressure and alcolol-related harm are mentioned, along with the benefit of having a more personalised approach to health.
The section on ‘Giving our children the best start in life’ (p.20) mentions healthier pregnancies, improved language acquisition, reducing parental conflict, improving dental health, protecting mental health and schools involvement, but infant feeding is not mentioned at all!
However, in the Parliamentary debate on the vision (Prevention of Ill Health: Government Vision) on 5 November, Alison Thewliss MP made the case for supporting breastfeeding by investing in the Baby Friendly Initiative to bring all maternity and community services up to the minimum standard. Matthew Hancock’s reply sounds positive: ‘The earlier that we can start with this sort of strategy of preventing ill health the better, and there is a lot of merit in a lot of what the hon. Lady said.’
‘Prevention, Protection and Promotion’ at Public Health England
Earlier in the year (March 2018), Professor Viv Bennett, the Chief Public Health Nurse, and Professor Jane Cummings, the Chief Nursing Officer, came together to launch a campaign on the ‘3Ps – Prevention, Protection and Promotion’, which is about actions to improve public health and reduce health inequalities. Breastfeeding is mentioned in the Maternity Transformation Campaign and Better Births and there appears to be increased govenment commitment to the key role breastfeeding plays in improving public health.
Directors of Public Health have a key role
The DHSC paper expects Directors of Public Health to ‘play an important leadership role’ (p.15). As an example, the Annual Report of Croydon’s Director of Public Health, published in mid-November, We are Croydon: Early Experiences Last a Lifetime, focusses this year on the first 1000 days of a child’s life.
It includes three breastfeeding recommendations:
Reset targets for increasing breastfeeding rates at 6 to 8 weeks and 6 months across the Borough and within particular localities
Achieve level 3 of the UNICEF Baby Friendly award
Turn Croydon into a breastfeeding friendly Borough, so women feel comfortable breastfeeding when they are out and about
How can progress on prevention occur unless it starts at the beginning – with infants? Will other Directors come up with similar recommendations?
Make London a ‘Baby-Friendly’ city
The Mayor of London, Sadiq Khan, aims to “make London a ‘Baby-Friendly’ city” in the London Food Strategy. This strategy aims to increase the health of all Londoners from infancy onwards, including supporting and normalising breastfeeding across London Transport and across government buildings and workplaces, and encouraging all London boroughs to become Unicef UK Baby Friendly-accredited in maternity and community services.
The UK government is due to publish a Green Paper on Prevention in 2019 to set out more detailed plans and, together with the NHS Long Term Plan, which is due to be published soon, is relevant to a future with better health for all.
What can YOU do?
Sign up for our mailing list and to volunteer in our campaigns here!
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group.
The First 1000 Days of Life (from conception to the age of two years) are a critical window in a baby’s development. The 1000 Days concept was first widely used by the World Health Organisation and UNICEF, and there are currently numerous campaigns building on that theme.*
A focused briefing on the the role of breastfeeding on infant brain growth and emotional development can be found here.
Breastfeeding: cornerstone of the First 1000 Days
Human babies are born extremely immature compared to other mammals; they are completely dependent on their mothers for milk, comfort and warmth.
“A newborn baby has only three demands. They are warmth in the arms of its mother, food from her breasts, and security in the knowledge of her presence. Breastfeeding satisfies all three.” ~ Grantly Dick-Read
Scientific research has continued to underscore the vital role that breastfeeding and breastmilk play in the development of the human infant. See our WBTi blog series for this year’s World Breastfeeding Week, from 31st July – 7th August 2018 for a review of the myriad ways that breastfeeding influences human development.
Breastfeeding: more than just food
This is the title of a series of blogs by Dr Jenny Thomas which focuses on some of the ways that breastfeeding contributes to immune development and more. Beyond physical health and development, however, breastfeeding also plays a key role in the healthy mental and emotional development of the infant. Breastfeeding provides optimal nutrition for the first months and years of life, alongside suitable complementary food after six months, but it also supports the development of the child’s immune system and protects against a number of non-communicable diseases in later life as well.
The World Health Organization commissioned high level reviews on a range of health and cognitive outcomes which were published in a special issue of Acta Paediatrica in 2015; these formed the foundation of the Lancet Series on Breastfeeding which was published in 2016.
The impact of breastfeeding on maternal and infant mental health and wellbeing.
Breastfeeding can help strengthen mother and baby’s resilience against adversity, and can protect infants even when their mothers suffer from postnatal depression. It supports optimal brain growth and cognitive development. Unfortunately, if mothers don’t receive the support they need with breastfeeding, this can significantly increase their risk of postnatal depression. A summary of evidence can be found here.
It is essential that policy makers, commissioners, and researchers understand the evidence and importance of breastfeeding, so that women who want to breastfeed get any support they need. The WBTI report outlines major policies and programmes that national infant feeding strategies need to include; other research on the psychological and cultural influences on mothers’ infant feeding decisions will help policy makers to develop sensitive and sound policies and programmes to support all families.
In the end, it will be essential that families themselves are heard, in order to create the support systems that our society needs.
*Unfortunately a number of infant milk and baby food companies have jumped on the “1000 Days” bandwagon too, despite the fact that breastfeeding is the centrepiece of the original 1000 Days concept, and replacing breastmilk with formula or baby food actually removes that fundamental building block from a baby’s development.
Helen Gray MPhil IBCLC is Joint Coordinator of the World Breastfeeding Trends Initiative (WBTi) UK Working Group. She is on the national committee of Lactation Consultants of Great Britain, and is also an accredited La Leche League Leader. She is a founding member of National Maternity Voices. She represents LLLGB on the UK Baby Feeding Law Group, and serves on the La Leche League International special committee on the International Code.
If you attended the 2015 Unicef UK Baby Friendly conference you may have noticed, or taken part, in the informal World Breastfeeding Trends Initiative (WBTi) competition to guess the final assessment score. Sue Ashfield is the winner as her estimate was closest to the actual score of 50.5 out of 100 for Indicators 1-10.
The score is a measure of how the UK is performing against the implementation of key policies and programmes to support mothers who want to breastfeed and the healthcare professionals who help them.
Sue is the lead and Specialist Health Visitor (Infant Nutrition) of First Community Health and Care in East Surrey. Sue is a winner in a much bigger way than the WBTi competition because her community team was reaccredited by Baby Friendly earlier this year and they also supported 10 local children centres in achieving full BFI accreditation in one year. The formal presentation of the award was on March 14th. Sue pays tribute to the hard work of her colleagues for the achievement but it also reflects her commitment and leadership. Read more here.
Her team is a brilliant example of what the WBTi UK report recommends for Indicator 6 (community-based support). There is close, integrated working between 0-19 public health team, breastfeeding counsellors, peer supporters and children centres at the three Baby Cafes, which have been runnning for 10 years.
Practitioners from the 0-19 team work at the Baby Cafes on a rota basis, alongside the breastfeeding counsellor. When they see mothers at home or at drop-in clinics they encourage them to attend the Baby Cafes for social support or more specialised support or just to chat to one of the peer supporters. The breastfeeding counsellors at the Baby Cafes have now trained over 200 peer supporters and this has increased the breastfeeding knowledge and skills within the local community.
Credit: Eleanor Stock
The photo above shows Sue holding the Baby Friendly Initiative (BFI) accreditation plaque along with some members of the 0-19 team, some senior managers and their BFI Guardian. Since April, all three community services in Surrey have come together as Children and Family Health Surrey to deliver children’s services.
Sue comments that she found particularly useful the information in the WBTi report about interventions and investment offered in the past and also Report Cards and the summary gaps and recommendations. She will use the findings in the report to inform local commissioners and disseminate information to staff and other stakeholders.
An integrated service like this is needed in all areas, yet in so many places services are being cut, particularly peer support programmes and breastfeeding support drop-ins.
Many congratulations Sue.
Cover photo credit: Paul Carter
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group
Will you be my Valentine? Love matters to all of us.
There will be millions of Valentine celebrations taking place all over the nation on 14 February. Hearts, red roses, chocolates, gifts, expensive treats and marriage proposals will be exchanged to signal love on that day.
But… babies are born every day. People embrace each other every day. Loving relationships begin every day! Lovers kiss every day and babies are universally loved.
Affection and love shape our brains from that first kiss on day one and continually along our life course. They create that extraordinary mother and baby bond, stimulate social interactions and enable long-lasting friendships. Early loving relationships are nurtured and supported by our families, friends, health professionals and wider society. Being held closely, and responded to sensitively, by those who love you more than anyone else, has far-reaching effects on long-term emotional security and health.
The Unicef UK Baby Friendly Initiative programme has been universal in changing attitudes and encouraging best practice over the last 20 years in the UK through robust accreditation. It delivers the minimum basic standards required to support new parents – no matter how they feed their babies. It aims to create the best environment for the start of every baby’s life but is not yet mandatory for all maternity facilities in England and Wales (see WBTi UK 2016 report – Part 1, Indicator 2).
The question is why isn’t it mandatory as recommended by NICE (the National Institute for Health and Care Excellence) 11 years ago? The guidance states: “All maternity care providers (whether working in hospital or in primary care) should implement an externally evaluated, structured programme that encourages breastfeeding, using the Baby Friendly Initiative as a minimum standard.”
The governments of Scotland and Northern Ireland have a funded national strategy with a coordinator supporting all maternal and infant health professionals, and 100% of maternity units in Scotland and Northern Ireland are accredited, with community facilities aiming to achieve the same.
This cascade of national to local support aims to ensure all parents receive the best possible information, free from the undermining effects of commercial persuasion, with practical support to be enabled to make healthy decisions for themselves, which helps fulfil the government’s health message.
Families would benefit if England and Wales followed the best practice example of their neighbours.
What does Baby Friendly care mean for parents? Relevant information from pregnancy onwards, skin-to-skin contact immediately after birth as standard practice, and practical help with learning how to feed your baby. For more details, see You can expect the following standards of care from aBaby Friendly hospital. If all expectant parents knew about the standards, they could help press for them to be implemented universally.
The WBTi UK report points out gaps and provides recommendations to overcome the many barriers that women face in their daily lives, journeying from pregnancy through birth, the postnatal months, back to work and beyond, living in their own communities. See Part 1, Indicator 2 of the report for more information, with further details in Part 2.
Implementing the WBTi recommendations would contribute to the provision of the optimal conditions all parents need to begin raising their child in a loving and supportive society.





























 Helen Gray MPhil IBCLC is Joint Coordinator of the World Breastfeeding Trends Initiative (WBTi) UK Working Group. She is on the national committee of Lactation Consultants of Great Britain, and is also an accredited La Leche League Leader. She is a founding member of National Maternity Voices. She represents LLLGB on the UK Baby Feeding Law Group, and serves on the La Leche League International special committee on the International Code.
Helen Gray MPhil IBCLC is Joint Coordinator of the World Breastfeeding Trends Initiative (WBTi) UK Working Group. She is on the national committee of Lactation Consultants of Great Britain, and is also an accredited La Leche League Leader. She is a founding member of National Maternity Voices. She represents LLLGB on the UK Baby Feeding Law Group, and serves on the La Leche League International special committee on the International Code.




{kind=link}