
It takes a village to raise a child – we all have a role to play to support breastfeeding mothers and babies.
We all are the building blocks responsible for supporting new families: partners and family members, health workers, neighbours and community members, religious leaders, employers, academics, governments and policy makers. We can all make a difference. We need to step up to our responsibilities. Everyone needs to understand the importance of breastfeeding – for maternal and infant physical and mental health and wellbeing, for public health, for our economy, and for our planet.
For WBW this year, WABA has produced an extensive suite of materials looking at all these roles and responsibilities. They have outlined the challenges that breastfeeding families face at every stage from conception, through birth, getting breastfeeding off to a good start, and maintaining breastfeeding all the way through starting solids and going back to work, and the solutions we need in each situation – all backed up by links to the latest evidence.
The #WBW2022 Action Folder pulls all this together: it is a useful resource for anyone using evidence to build policies and best practice. You can download it as a PDF and all the links to research and references will be live.
The UK WBTi team will be highlighting just a few of the concepts this week:
- Health workers: the importance of relevant, evidence-based. The advertising of follow-on milks, on the media, from 6 months in the UK has led to confusion, resulting in some parents seeing formula milk as equivalent to breastmilk, or that breastfeeding should stop at 6 months. The International Code needs to be adopted by the UK government in full, to reduce this confusion and protect breastfeeding. training for all those who work with women, infants and young children
- UNICEF UK Baby Friendly Initiative and the BFHI worldwide sets out ways in which healthcare staff can receive sound, evidence-based, basic training in supporting breastfeeding.
ALSO join a special webinar from the Global Breastfeeding Collective on BFHI, with some added specialist topics on supporting small and underweight breastfeeding infants, and on infant feeding in emergencies. (7-9 AM BST and again at 4-6 PM BST). Register HERE
- Community support: Access to skilled, integrated support for all, with a special focus in the GBC webinar on how to support breastfeeding infants who are not gaining well (NICE NG 75,2017). All parents should have easy access to trained healthcare staff- midwives, paediatricians, health visitors and GPs- breastfeeding peer supporters and specialist support (IBCLC, BFCs). Supporting breastfeeding in complex circumstances: Specialist support from IBCLCS, BFCs, or infant feeding leads, integrated with specialist healthcare teams
- Protecting infants and young children in emergencies. National policies should guide Local Resilience Forums but these do not exist at present.
- The impact of misleading marketing: The International Code. The advertising of follow-on milks, on the media, from 6 months in the UK has led to confusion, resulting in some parents seeing formula milk as equivalent to breastmilk, or that breastfeeding should stop at 6 months. The International Code needs to be adopted by the UK government in full, to reduce this confusion and protect breastfeeding.
- Governments with national and local policy makers need to protect all families and support them to make informed feeding decisions free of commercial influence.
What can YOU do?
It is time for a reassessment of the UK’s national infant feeding policies and programmes. YOU could help! Volunteers are welcome with knowledge in any of the ten policy areas (Indicators 1-10), or with skills such as research, writing, graphics, social media and more – feel free to contact us for a chat!
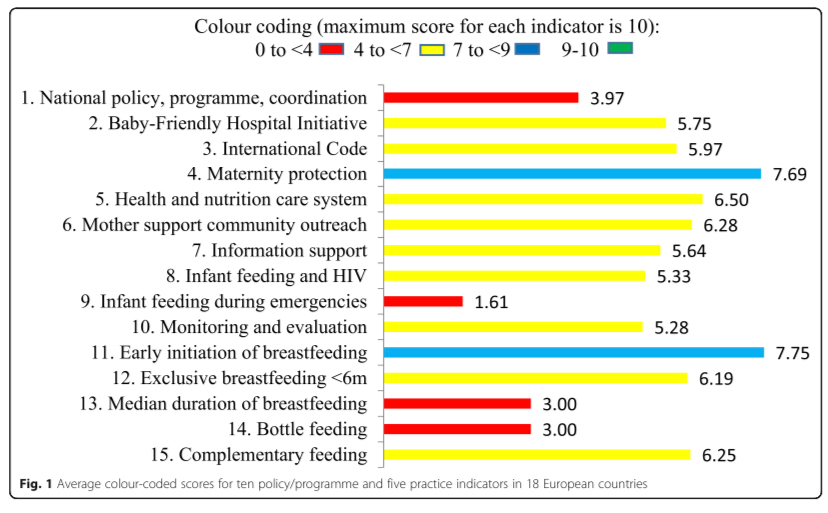
WBTi Key Indicators:
Indicator 1: National policy, programme and coordination
Indicator 2: Baby Friendly Initiative
Indicator 3: International Code of Marketing of Breastmilk Substitutes
Indicator 4: Maternity protection
Indicator 5: Health professional training
Indicator 6: Community-based support
Indicator 7: Information support
Indicator 8: Infant feeding and HIV
Indicator 9: Infant and young child feeding during emergencies
Indicator 10: Monitoring and evaluation
Which one will YOU choose?
Contact us: wbti@ukbreastfeeding.org























 Helen Gray MPhil IBCLC is Joint Coordinator of the World Breastfeeding Trends Initiative (WBTi) UK Working Group. She is on the national committee of Lactation Consultants of Great Britain, and is also an accredited La Leche League Leader. She is a founding member of National Maternity Voices. She represents LLLGB on the UK Baby Feeding Law Group, and serves on the La Leche League International special committee on the International Code.
Helen Gray MPhil IBCLC is Joint Coordinator of the World Breastfeeding Trends Initiative (WBTi) UK Working Group. She is on the national committee of Lactation Consultants of Great Britain, and is also an accredited La Leche League Leader. She is a founding member of National Maternity Voices. She represents LLLGB on the UK Baby Feeding Law Group, and serves on the La Leche League International special committee on the International Code.

