“Breastfeeding is a matter of human rights for both mothers and children,” say United Nations experts in an unprecedented joint statement today. Gaps identified by the UN mirror many of the gaps identified in the recently published World Breastfeeding Trends Initiative (WBTi) report on the state of breastfeeding in the UK, specifically:
Gaps in knowledge and skills among healthcare providers (WBTi Indicator 5)
Lack of access to accurate information or support (WBTi Indicators 6 and 7)
Family, community, and cultural practices and traditions that are not necessarily pro-breastfeeding (WBTi Indicator 7)
Limited or non-existent maternity protection in the workplace (WBTi Indicator 4)
Misleading marketing of breastmilk substitutes, and the lack of corporate accountability for the adverse consequences of such marketing practices (WBTi Indicator 3)
In cases where a woman cannot breastfeed or is not willing to do so, even after having been duly informed about the benefits of breastfeeding, access to good quality breast milk substitutes should be regulated and affordable, without condemnation or judgment (WBTi Indicators 3, 5, 7)
Investments to support breastfeeding are often marginal and far from adequate (WBTi Indicator 1)
Previous UN recommendations specific to the UK also included the recommendation to systematically collect data on infant and children’s food and diet (WBTi Indicator 10).
Human rights, and the UK’s obligations under the Convention of the Rights of the Child, underpin the WBTi UK Report, which states: “The mother and the baby are a dyad, and they have rights as a dyad; [neither trumps the other]. Each has explicit rights; both mother and baby require protection and support to make successful breastfeeding a reality.”
UN Special Rapporteurs on the Right to Food, Right to Health, the Working Group on Discrimination against Women in law and in practice, and the Committee on the Rights of the Child issued the statement through the Office of the United Nations High Commissioner for Human Rights today.
Do you want to help bring about real changes to breastfeeding in the UK? If so, read on, because every baby born in this country needs your help.
Write to your MP to ensure that the All Party Parliamentary Group on infant feeding gets off the ground
If you’ve been a regular on the UK Breastfeeding blog then you’ll know all about the WBTi, and how it is identifying every aspect of breastfeeding policy and practice that is falling short and generating recommendations for how they can be improved.
But how can we make sure that those recommendations get put into practice? That’s where you come in – by influencing your MP and making sure they understand that this issue is important to you and to thousands of other families in their constituency.
In November, the WBTi steering group was delighted to be invited to the first-ever meeting of the All Party Parliamentary Group for Infant Feeding and Inequalities. This was organised by Alison Thewliss MP, who is as committed as we are to bringing about real improvements to infant health through breastfeeding.
All Party Parliamentary Groups are an excellent way to educate and inform interested MPs, who can then take questions to the floor of the House of Commons, help to push issues to the top of the political agenda, and hold government ministers to account. There are APPGs for every subject under the sun, but until now there has not been one dedicated to infant feeding, which affects every baby in this country!
At the meeting in November, Helen Gray and Clare Meynell gave an excellent presentation on the WBTi project, explaining why politicians should care about breastfeeding and how current practices result in so many mothers stopping breastfeeding much earlier than they wanted to.
But, by the time they had begun their first slide, Alison Thewliss was the only MP still in the room!
Clearly, we need more MPs to come along and listen to these important messages and to push for change on behalf of the mothers and babies in their constituencies and around the country.
So please spare 5 minutes to write to your MP to make sure they attend the next meeting (for MPs only), which is on Tuesday 19th January at 9.30am in Room W1 of Westminster Hall. Can you spare those few moments to help make a difference?
As MPs are more likely to respond to your own letter than to a standard letter, the best approach is to adapt the short letter below using your own words. If you can add information about your own experience and why you think the APPG is needed, that would have even more impact.
It is essential to include your name and address (and postcode) as MPs can only respond to requests from their own constituency.
Once you have identified who your local MP is, send them the following message. Remember to include your full name and postcode.
Please feel free to send us any response you receive from your MP.
Model letter (please adapt):
Dear [insert MP’s name]
As my local MP, I am writing to ask if you will represent me, and an interest close to my heart, in the House of Commons?
There have been efforts to establish an All Party Parliamentary Group on Infant Feeding & Inequalities in the UK Parliament. Although the group tried to form in November, I understand that there wasn’t enough cross-party representation, particularly from Conservative and Labour MPs. I was really disappointed to learn that this actually prohibited the group from getting off the ground.
However, I gather that there is another short meeting for MPs to establish the APPG on Tuesday 19th January at 9.30am in W1 of Westminster Hall.
Will you attend the meeting on my behalf and ensure this group gets off the ground? Will you add your name to join the group?
There are so many important discussions and campaigns which should be considered around the area of infant feeding, and I would be delighted if you, as my MP, could attend and help raise this issue on my behalf.
Today is World Aids Day, so what better time to look at the issue of breastfeeding and HIV? Indicator 8 of the World Breastfeeding Trends initiative (WBTi) examines what policies countries have in place to protect HIV-positive mothers and their babies.
Read what the World Alliance for Breastfeeding Action has to say today on this important topic.
Thirty years since the first report appeared documenting transmission of the Human Immunodeficiency Virus (HIV) through breastfeeding, breastfeeding by HIV-Positive mothers has never been as safe as it is now in 2015. So long as several easily achievable conditions are fulfilled, the risk of transmission of the virus through mother’s milk can be reduced to almost zero (0-1%). [Read more…]
74 percent of mothers initiated breastfeeding 44 percent of mothers were still breastfeeding at 6–8 weeks
– Public Health Outcomes Framework (England) 2014/15
90 percent of women who stop breastfeeding in the first six weeks report giving up before they wanted to
– David Bull, Executive Director UNICEF UK
Most mothers in the UK want to breastfeed, yet most mothers stop breastfeeding before they want to. Why?
The fact is that while breastfeeding is natural, mothers need skilled support to be able to breastfeed. Yet many of the health professionals who work with mothers and babies do not have the knowledge or skills to help them.
Indicator 5 of the WBTi examines how well healthcare systems support breastfeeding. It looks in detail at the training of all health professionals who interact with mothers and babies – midwives, health visitors, GPs, paediatricians, lactation consultants and others – both before and after they qualify in their profession. You can see the full education checklist here.
Support for mothers comes from many sources, not just health professionals. It can come from family, friends, the community at large, and particularly breastfeeding peer-support groups. In the UK, these are run by organisations like the Association of Breastfeeding Mothers, Breastfeeding Network, La Leche League, NCT, as well as by the NHS itself. Mothers who have breastfed their own babies – and who have received training to provide breastfeeding support – are able to provide valuable help to new mothers.
In the UK, just 1 percent of babies are exclusively breastfed for the recommended six months. Common reasons that mothers give for stopping breastfeeding include:
finding breastfeeding painful
concerns about their milk supply
conflicting advice from health professionals
lack of support
Trained support is needed at all levels, from peer supporters to lactation consultants. Click here for details of the different roles.
Peer supporters are “informed friends” who can help mothers understand what’s normal and help with many common breastfeeding concerns. They offer a compassionate and empathetic ear to new mothers.
This importance of this community-level support is recognised in Indicator 6 of the WBTi, which looks in detail at access to skilled mother support and community outreach. Good peer-support programmes can increase the length of time that mothers exclusively breastfeed their babies. In other words, they can help mothers who want to breastfeed to carry on for as long they choose.
When the Industrial Revolution began, women started to go out to work in large numbers and breastfeeding began to decline, spurring the development of alternative ways of feeding babies. Yet, 200 years on, the question of how to combine breastfeeding and work still remains for women around the globe.
In the UK in 2015, MPs themselves are struggling to secure the right to breastfeed their babies in the chamber of the Houses of Parliament itself!
Once again, the Global Strategy on Infant and Young Child Feeding is clear that there are proven ways to make this work. It calls on governments to produce “imaginative legislation” to protect the breastfeeding rights of working women.
health protection, job protection and non-discrimination for pregnant and breastfeeding workers
at least 14 weeks of paid maternity leave
one or more paid breastfeeding breaks or daily reduction of hours of work to breastfeed
as well as recommending that space be provided nearby for working mothers to breastfeed or express their milk.
There is also a recognition of the extra challenges faced by women who work in the “informal economy”, such as those in casual or freelance work, who don’t always have the same protections as other women.
Each year, the World Alliance for Breastfeeding Action produces a snapshot of the state of maternity protection around the world, which makes for some interesting comparisons.
WABA 2015
Indicator 4 of the World Breastfeeding Trends initiative (WBTi) looks in much more detail at the laws and practices in each country to score them on the maternity protection they offer. Fathers are recognised too, because of their important role in nurturing babies and supporting breastfeeding, so the length of paternity leave is also included in the score.
How do you think the UK compares to other countries in protecting breastfeeding mothers at work? What was your experience of returning to work while breastfeeding? What would have made it easier?
A baby is born and placed on his mother’s chest. His newborn reflexes kick in and he starts to crawl to her breast, calm and alert. This skin-to-skin contact triggers a surge in oxytocin – the so-called “mothering hormone” – and she responds by instinctively helping him to the breast. He latches on, and her milk flows.
When breastfeeding begins in this uninterrupted way, soon after birth, research shows that babies are more likely to breastfeed well, and mothers tend to continue to breastfeeding for longer.
Now compare this to the typical birth scenario, repeated in so many maternity hospitals:
A baby is born, and her cord is cut. The midwife announces “It’s a girl!” and then wipes the baby clean and wraps her up. Then she passes her to her mother. Then the baby is passed to her father. After a few minutes, the midwife unwraps the screaming baby and puts her on the scales and gives her a vitamin K injection. The baby is dressed and returned to her mother.
There is clear evidence for better outcomes for babies born in Baby Friendly hospitals – for example, a study in Scotland found that these babies are 28 percent more likely to be exclusively breastfed at 7 days old.
The meaning of Baby Friendly has also evolved over time, and in recent years it has moved beyond the ten steps. In the UK, as well as protecting breastfeeding, the Baby Friendly approach now helps mothers to begin a nurturing relationship with their baby – and this protection applies to all babies, whether or not they are breastfed.
The Baby Friendly Initiative has also moved beyond maternity hospitals. In the UK, it is now possible for university courses, health visitors, children’s centres, and neonatal units to become Baby Friendly accredited.
The World Breastfeeding Trends initiative (WBTi) assessment scores each country out of 5 based on how many Baby Friendly hospitals it has. It needs have more than 89 percent of its hospitals and maternity units accredited to gain the top rating.
The assessment also looks at the quality of the Baby Friendly programme – how comprehensive the training is, whether it monitors hospitals adequately, whether mothers’ experiences are taken into account – for another possible score of 5.
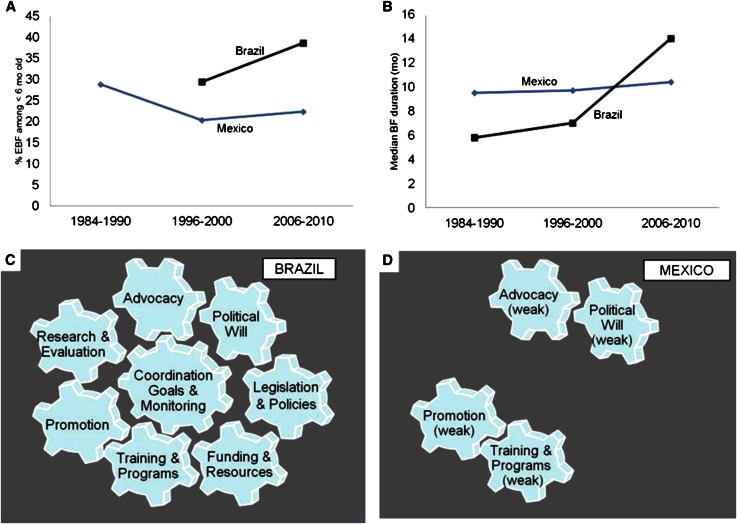
In the first presentation, this graphic popped up, and a collective “ooh” and then an “aah” went round the room. You may be forgiven for wondering why it generated such a response – it doesn’t look particularly inspiring!
Credit: Pérez-Escamilla et al, Advances in Nutrition, Nov 2012
It’s because this picture demonstrates what happens when there is a strong national strategy on breastfeeding – and also what happens when there isn’t.
In the late 1990s, Brazil made a concerted effort to improve infant health through a drive to increase breastfeeding rates in the country. They put in place legislation to protect mothers, training for health professionals, breastfeeding promotion – along with the money to pay for it all. And they had a national coordinated breastfeeding strategy to make it happen.
At the same time, Mexico had no such national strategy. Half-hearted efforts were made in some areas, such as training for health professionals and public promotion of breastfeeding.
As the graphs show, Brazil was able to significantly increase breastfeeding rates over that period while in Mexico they stagnated.
Without a strong, national, coordinated breastfeeding strategy to drive things forward, everything else is just wheels turning in the wind.
That’s the metaphor – what does this all mean in practice for the UK?
Let’s imagine a mother, who has her baby in a Baby Friendly hospital [1] and breastfeeding gets off to a good start. But then she arrives home and starts to experience some problems. Her health visitor suggests she gives the baby some formula [2]. She’s seen some adverts on television and buys a particular brand of formula because it’s “closer to breastmilk” [3]. She lives in a rural area, and the nearest breastfeeding support group is 10 miles away and she doesn’t drive [4]. Her husband has seen the adverts too so he knows that “good dads do the night feeds” [5]. After a couple of weeks the baby is getting more and more formula and is breastfeeding less and less. Her husband suggests she’s given breastfeeding a good go but maybe she should stop now [7]. She had wanted to breastfeed for longer but she gives up [8].
Indicator 2 of the WBTi asks – are babies born in Baby Friendly hospitals?
Indicator 5 asks – do health professionals have adequate breastfeeding training?
Indicator 3 asks – is the International Code of Marketing of Breastmilk Substitutes fully implemented?
Indicator 6 asks– do all mothers have access to breastfeeding support in the community?
(see Indicator 3)
Indicator 7 asks – do parents have access to good information about breastfeeding and the risks of using formula?
Indicator 12 asks – what percentage of babies are exclusively breastfed for the first six months?
Without this central cog (Indicator 1) driving all the other cogs (Indicators 2-10) things cannot move forward. This point is also made clear in a new report from Save the Children, which looked at breastfeeding policies and practices in six countries, including the UK.
there needs to be a National Breastfeeding Committee
that committee must meet on a regular basis to review progress
that committee needs to link effectively with public health bodies
that committee must have a coordinator who communicates national policy at regional and local levels
Indicator 1 of the WBTi assessment asks whether a country has each of the above and gives a total score out of 10. How well do you think the UK as whole will score? How would the countries of the UK score individually? What do we need to do to improve that score? How can policies be turned into actions at a local level?
In the next blog post we will be talking about Indicator 2 – Baby Friendly care and Baby-Friendly Hospital Initiative and will be asking for your thoughts about how things can be improved.
Don’t be fooled by the uninspiring acronym – the WBTi is the most exciting thing to happen in breastfeeding in the UK for years!
The name stands for the World Breastfeeding Trends initiative and it was launched in 2005 by IBFAN, and the idea is to take a snapshot of breastfeeding in a country – the policies, practices and breastfeeding rates – and then (and this is the important bit) to create some recommended actions to improve things.
The assessment is then repeated 3 to 5 years later and a new set of recommendations are made. The idea is to create an upward trend of continuing improvements over time so that more babies are breastfed and for longer, improving infant and maternal health.
Governments don’t need to keep reinventing the wheel because we already know what works. Back in 2003 the WHO produced (and member countries signed up for) the excellent Global Strategy on Infant and Young Child Feeding, which outlines exactly what they need to do to improve breastfeeding rates. It says that:
· All governments should develop and implement a comprehensive policy on infant and young child feeding.
· All mothers should have access to skilled support to initiate and sustain exclusive breastfeeding for 6 months and ensure the timely introduction of adequate and safe complementary foods with continued breastfeeding up to two years or beyond.
· Health workers should be empowered to provide effective feeding counselling, and their services be extended in the community by trained lay or peer counsellors.
· Governments should review progress in national implementation of the International Code of Marketing of Breast-milk Substitutes, and consider new legislation or additional measures as needed to protect families from adverse commercial influences.
· Governments should enact imaginative legislation protecting the breastfeeding rights of working women and establishing means for its enforcement in accordance with international labour standards.
The WBTi breaks down the Global Strategy into 10 areas (indicators) and asks a short set of pertinent questions to see how the country is doing in each one. Where gaps are identified, recommendations are put forward to fill them.
Studies show that countries that have enacted the Global Strategy – in all 10 areas, not just a select few – have seen great improvements in their breastfeeding rates.
Over 100 countries are involved in the WBTi but this is the first time for the UK. The beauty of the process is that it is a collaborative effort between government officials and organisations involved in breastfeeding. If you are a mother, peer supporter, midwife, health visitor or lactation consultant – we’d also like to get your views. Over the coming days we’ll be posting a key question for each Indicator and will be asking what actions you think the WBTi should recommend in its report. So stay posted…
The meeting brings together key breastfeeding organisations in the country to complete the first UK WBTi assessment, a detailed exercise that will result in a “report card” on breastfeeding for the UK. This will give a clear picture of the state of breastfeeding – both policies and practices – in the UK.
The partner organisations will then put forward a plan highlighting what actions to take to address the gaps identified.
The WHO Global Strategy recognises that for breastfeeding to be successful mothers and families need the right support along the whole course of breastfeeding – from giving birth in a Baby Friendly hospital, to going home to find skilled local support from midwives, health visitors, GPs, and mother support groups throughout their communities. After that they need maternity protection and breastfeeding breaks when they return to work. They need accurate information about breastfeeding – without marketing pressure from formula manufacturers – from friends, family and the media, as well as health professionals and policymakers.
Those countries that have enacted the WHO Global Strategy have seen marked improvements in breastfeeding rates. For example, a recent report by Save the Children looked at breastfeeding policies and practices in six countries, including the UK, and highlighted the importance of a strong national policy on infant feeding.
The UK meanwhile has some of the lowest breastfeeding rates in the world. Only 1% of babies are exclusively breastfed for six months, despite recommendations by WHO and Department of Health.
The partner organisations involved in WBTi UK assessment include: Public Health Wales, Public Health England, CHIMAT, CPHVA, Institute of Health Visiting, Nursing and Midwifery Council, National Infant Feeding Network, UNICEF Baby Friendly UK, Baby Feeding Law Group, Lactation Consultants of Great Britain, Association of Breastfeeding Mothers, Breastfeeding Network, La Leche League GB, NCT, Best Beginnings, IBFAN Baby Milk Action, Maternity Action and First Steps Nutrition Trust.