Position Statement On Breastfeeding From The RCPCH
Today is the start of World Breastfeeding Week. An open letter was published in The Guardian today, from the Royal College of Paediatrics and Child Health (RCPCH), co-signed by the WBTi team and 17 other organisations working in maternal and infant health. The letter calls for improved social attitudes towards breastfeeding to help reduce the barriers so that women are more able to sustain breastfeeding.
The revised RCPCH position statement on breastfeeding, also launched today, points out the rapid decline in breastfeeding rates (leading to fewer than half of all babies receiving any breastmilk at all by 6-8 weeks after birth), the research evidence on improved health outcomes and intelligence scores, and the economic impact. It lists key messages for health professionals and recommends government action to increase initiation and continuation rates. Roles and responsibilities of paediatricians include:
“All paediatricians should be aware of the RCPCH position on breastfeeding and encourage and support mothers, including those with preterm or sick infants, to breastfeed. They should avoid undermining breastfeeding through the inappropriate use of infant formula “top-ups”, and advise women that the use of infant formula may make it more difficult to establish exclusive breastfeeding.”
While the position statement mentions that the current training curriculum for general paediatricians “requires trainees to understand the importance of breastfeeding and lactation physiology, be able to recognise common breastfeeding problems”, the WBTi assessment found significant gaps in comparison to the WHO Education Checklist for infant and young child feeding topics. However, the curriculum is currently being revised and we very much hope this will improve such training for paediatricians.
Family-centred care
Indicator 5 in the WBTi UK report is about health and nutrition care systems.
Are the services provided by maternity units truly mother- centred? Are health professionals such as health visitors, GPs and relevant hospital staff, with an in-patient mother, baby or young child, really mother centred?
To achieve parent-centredness, the policies and protocols need to incorporate that ethos, and staff training needs to provide the necessary attitudes, knowledge and skills. The crucial element of Indicator 5 is, therefore, health professional training.
Training for health professionals
Our report showed significant gaps in training for most of the relevant professions. Those who support mothers with breastfeeding have much anecdotal evidence between them of extensive variation between health professionals in attitudes and knowledge, from being hugely supportive on the one hand to dismissive of breastfeeding on the other. If all had a positive attitude towards breastfeeding, accompanied by basic knowledge, that would surely help to improve breastfeeding rates, particularly for continuation?
Time for action
The recommendations by the WBTi Core Group mirror those of the RCPCH – action is needed at every level, from governments to health professional bodies. from the community to the workplace. Protecting our babies’ future is a responsibility we all share.
Key gaps and recommendations from the 2016 World Breastfeeding Trends Initiative report on UK infant feeding policies and programmes https://ukbreastfeeding.org/wbtiuk2016/
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group
The World Breastfeeding Trends Initiative UK Report in 2016 includes the statements that “employment tribunal fees were introduced in 2013 (except in Northern Ireland) and it now costs £1200 to bring a discrimination claim. Employment tribunal fees constitute a significant financial barrier to accessing justice. The number of employment tribunal claims decreased by 70% following introduction of the fees.”
The unanimous recommendations by the WBTi Core Group organisations included:
“that governments ensure that tribunal access is available to women from all income brackets.”
Tribunal fees ended with immediate effect
The excellent news is that on 26th July 2017 the UK Supreme Court ended employment tribunal fees with immediate effect. The Parliamentary Justice Committee had recommended special consideration for pregnancy and maternity discrimination claims in 2016 but as no government action followed, the trade union Unison took the issue to court. Rosalind Bragg, Director of Maternity Action, has written about this in more detail:
The Press summary of the judgment explains that “The Fees Order is unlawful under both domestic and EU law because it has the effect of preventing access to justice. ” It indirectly discriminates against women under the Equality Act 2010 because more women make Type B claims, which include unfair dismissal, equal pay and discrimination.
Another change to improve access to justice that is listed in the Plan is to extend the timeline for making a claim from 3 months to 6 months. Joeli Brearley set up Pregnant then screwed to tackle employment discrimination and her #GivemeSix petition aims to achieve this extension so that mothers can begin a tribunal claim after they give birth and avoid risking extra stress in pregnancy. The Early Day Motion (EDM15) to increase the time limit has been signed by 87 MPs so far, approaching the target of 100.
Guidance is needed on infant and young child feeding for families in the UK affected by disasters and emergencies.
Heather Trickey and Helen Gray.
Disaster and emergency situations – floods, fires, terrorist attacks and widespread power failures – can affect any country, including the UK. In any disaster or emergency, babies are vulnerable and continued access to adequate and safe nutrition is essential. Families need support to ensure that children continue to be cared for and fed in line with their needs.
There is no UK government plan
The World Health Assembly (WHA Resolution 63.23) has recommended that all countries implement existing global guidelines on infant feeding during emergencies, including specific operational guidance to help relief agencies protect infant nutrition and minimise risk of infection. Although there is national guidance on care of animals during emergencies, a recent World Breastfeeding Trends Initiative (WBTi) report found that there are no UK-wide or national strategies addressing infant and young child feeding during a disaster. Scotland is the only part of the UK that has a named lead on infant feeding in emergencies. Emergency planning and response is devolved to local authorities; because there is no guidance on the protection of families with infants there is no way to ensure that local strategies consider infant nutrition as part of emergency response.
Risks for formula fed babies
Babies who are fully or partially formula fed are at risk if their caregivers lose access to clean water, are unable to sterilise feeding equipment or suffer disruption or contamination of their formula milk supplies. A suitable environment for preparation and storage of feeds, sterilising equipment, boiling water and safe storage such as a refrigerator, are all needed to prevent bacterial contamination
Emergency supplies required to care for and feed a formula fed baby for one week in a developed country, using read-to-feed milk. From Gribble & Berry 2011 “Emergency Preparedness for those who care for infants in developed country contexts.” International Breastfeeding Journal /2011 6:16
Risks for breastfed babies
Breastfeeding protects against infection and can be comforting to infants and mothers during difficult times. Mothers’ supply of breastmilk is resilient, however, chaos, displacement and emotional strain, coupled with commonly held misconceptions about how breastfeeding works, can undermine a mother’s confidence and result in less frequent feeding. Breastfeeding mothers need access to the option of feeding in a private space and reassurance that continuing to breastfeed is the best option for their baby.
Skilled support can help mothers resolve breastfeeding problems and maintain the protective effect of full or partial breastfeeding. If breastfeeding helpers are not pre-authorised as part of planned disaster response the immediate help that families need can be delayed.
Risks associated with donated formula milk
The world is a better place than we sometimes think. When a disaster strikes, ordinary people often respond with an outpouring of generosity. We give clothes, equipment and food spontaneously and in response to public calls.
Donations of clothing, bedding, toys, food and water, London, June 2017. Photo Credit: @balhammosque
In the absence of guidance, agencies responsible for co-ordinating emergency response and volunteers working on the front line are often not aware that donations of formula milk can put babies at risk. Risks from donated formula milk include inadvertently distributing products that are unsuitable for babies under six months or for babies with special nutritional needs, as well as distributing milk that is contaminated or out-of-date. There is also a risk that donations will be inappropriately provided to parents of breastfed babies, which can undermine the protective effect of breastfeeding and cause parents to become dependent on a continued supply of formula milk.
International guidelines for emergency feeding caution against accepting donations of formula milk. It is recommended that emergency planners and first responders, with expert advice, take responsibility for purchase and distribution of appropriate formula milks in line with the needs of each family.
What’s been done so far?
International guidelines for protecting infants in disasters and emergencies are available. There is a need to adapt these to a UK context, where, beyond the early weeks, many babies are fully or partially formula fed and which includes a rich mix of cultures and nationalities with different feeding practices.
UK-based emergencies have tended to be highly localised and short-term. However, UK guidance will need to ensure preparedness for longer-term support needs, for UK charities and for displaced families and unaccompanied children who have sought refuge from outside of the UK.
Several UK agencies have developed guidance with limited scope. The Food Safety Agency has issued guidance to support safe preparation of formula milk in response to flooding and contamination of local water supplies. [20222 update: UNICEF UK Baby Friendly Initiative has produced guidance for Local Authorities on supporting families with infants who are experiencing food insecurity]
[2021 update: See also the infographic series from the Infant Feeding in Emergencies Core Group on managing appropriate infant feeding interventions during emergencies, including Preventing and managing inappropriate donations during emergencies: https://www.ennonline.net/ifecoregroupinfographicseries]
How to help ensure babies’ nutritional needs are protected
In the absence of national guidance, relief co-ordinators and agencies and members of the public will be concerned to do the right thing in response to a disaster. There is an urgent need to improve planning and raise awareness about the best ways to support infant and child feeding. These key points from have been adapted from UK and international guidance:
1) Members of the public
DO donate money to key agencies. This is the best way to support parents who need to buy formula milk. Money will allow parents, caregivers or coordinating aid organisations to buy the most appropriate milk to meet the individual needs of each baby. Donated formula milk can inadvertently put babies at risk.
DO offer your time to help agencies co-ordinating relief. Support and encourage mothers who are breastfeeding. Breastfeeding is protective against infection, and provides the baby with the safest possible nutrition.
2) Relief workers and aid agencies
DO have a local plan to support infant and young child feeding in emergencies in place for local authorities, first responders and aid agencies. All families should be screened to ensure they receive appropriate support or supplies.
DO ensure that mothers who are fully or partially breastfeeding have the support they need to continue. Mothers can seek support from their midwife or health visitor. Local emergency planning should have identified appropriate infant feeding support from local health and voluntary services. There are telephone helplines which support caregivers with all aspects of infant feeding:
NCT helpline (0300 330 0700)
The National Breastfeeding Helpline (0300 100 0212).
DO encourage donations of money to recognised agencies so that parents, caregivers and agencies can buy any formula or supplies needed, rather than donations of formula products.
Appropriate support or supplies including cash cards specifically for the purchase of infant formula and complementary foods for young children could be considered.
DO ensure that formula milk is purchased and distributed only for babies who need formula milk, following basic screening of families (simple triage tools have been recently been developed for use in emergency situations in Greece and Canada).
DO NOT distribute formula milk in an untargeted way.
DO ensure that parents are aware of guidance on sterilisation of bottles and teats and how to prepare any powdered formula safelyand have access to facilities to carry this out, to reduce the risk of contamination. Liquid ready-to-feed formula may be needed if suitable preparation facilities are not available.
What is needed now?
There is an urgent need for UK governments to ensure infant and child nutrition is protected as part of the planned new strategy for resilience in major disasters. Local authorities and relief agencies require national guidance to develop local strategies so that we can all be better prepared.
Heather Trickey is a Research Associate based in DECIPHer, Cardiff University. Her research focuses on public health policy and parents, particularly Infant Feeding Policy.
Helen Gray is Joint Coordinator of the World Breastfeeding Trends (WBTi) UK Working Group.
Doctors have to acquire a huge body of knowledge during training and for general practitioners that knowledge is particularly wide-ranging. Their ten or more years of study comprise undergraduate, foundation and specialism levels of training. As qualified GPs they are likely to have thousands of women patients who, at some stage, are breastfeeding mothers, yet the breastfeeding content of the curriculum is minimal.
Placements in the specialism training may offer useful opportunities to learn from midwives and health visitors about the practicalities of supporting breastfeeding but this is a matter of luck, and the knowledge and skills of those mentors can be variable. It would be much more effective to have a requirement for acquiring basic knowledge and skills specified in the curriculum as well.
GP Infant Feeding Network and resources for GPs
A number of GPs, mothers who in breastfeeding their own babies became acutely aware of the deficiencies in their training, set up the GP Infant Feeding Network, GPIFN, in February 2016. In April 2017 they launched the GPIFN website, a valuable resource for doctors.
Does your doctor know about this website?
Medical training
With regard to medical training (not just GP training), the General Medical Council (GMC) has recently published its Generic Professional Capabilities (GPC) Frameworkto provide broad outcomes for a consistent approach for postgraduate curricula. The framework was developed in partnership with the Academy of Medical Royal Colleges. Domain 4 (there are 9 domains) looks to be particularly relevant to protecting and supporting breastfeeding as its title is ‘Capabilities in health promotion and illness prevention’.
Royal colleges, such as the Royal College of General Practitioners (RCGP), are responsible for the details of their curricula. They revise them every few years and from the next revision will need to fit with the GPC Framework to be approved by the GMC.
The current standards show several gaps when evaluated by the WHO Education Checklist on infant feeding in the 2016 WBTi assessment of the UK.
Further information about standards for the different health professions can be found in Indicator 5 in Part 2 of the 2016 WBTi report.
Are you a doctor or trainee doctor?
If so, you might like to contact your specialty college asking for the infant feeding content of the curriculum to be improved.
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group, being the lead for Indicator 5, which is primarily about health professional training.
Peer Supporter, West Hertfordshire Hospitals NHS Trust
As a mum embarking on a new breastfeeding journey with their baby, who could she turn to for support and advice that she can trust? How would she know that what she’s doing is “right”, that her baby’s behaviour is “normal”? Her midwife? GP? Obstetrician? Paediatrician? Health Visitor? Surely the advice and support you get from a qualified and trained healthcare professional can be trusted? The findings from the World Breastfeeding Trends Initiative (WBTi) UK 2016 Report (published November 2016) may surprise you.
Health professional training in the UK
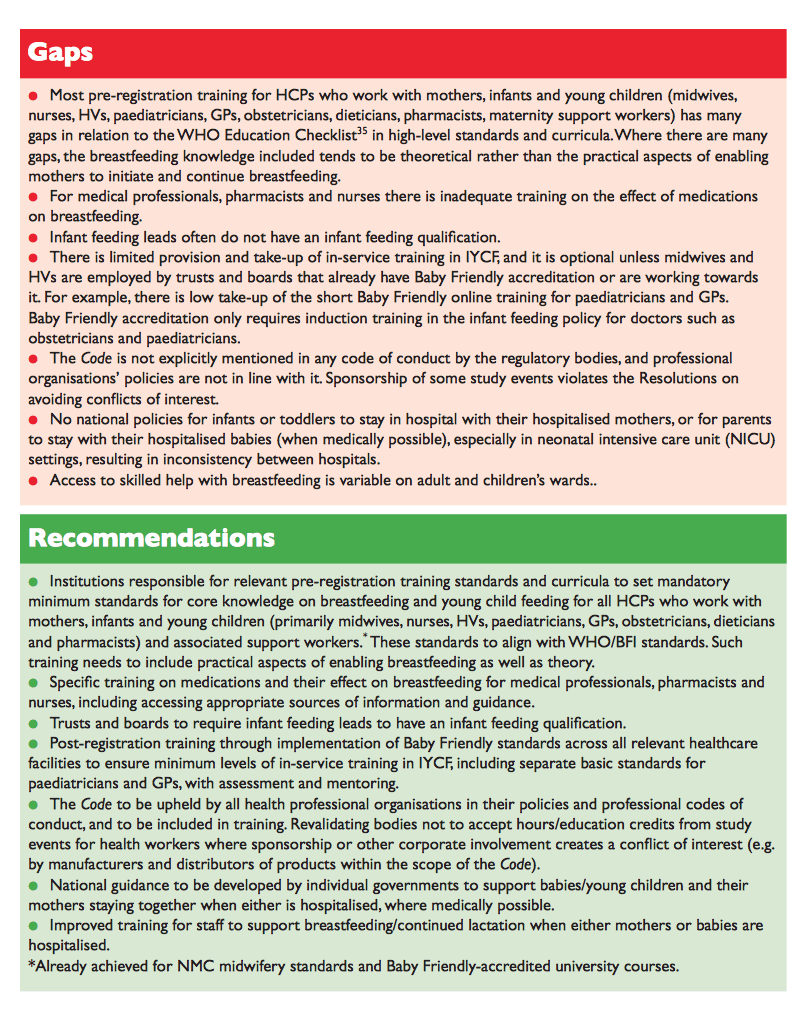
The WBTi UK Report (WBTi UK 2016) was based on the WBTi toolkit developed by the International Baby Food Action Network (IBFAN) to help countries evaluate breastfeeding policies and practices in a systematic way. One area that the report focuses on is health professional training and subsequent impact on breastfeeding initiation and continuation rates across the UK. Worryingly the report highlights many gaps in the pre-registration training of some healthcare professions in the area of infant and young child feeding, particularly in the practical aspects of enabling mothers to initiate and continue breastfeeding. Following qualification, healthcare professionals are then expected to undertake in-service training in infant and young child feeding. The WBTi UK Report reveals that provision and uptake of these courses is limited.
So what does this mean? The very healthcare professionals our new mums ought to be able to trust to give them the right advice may not be the right source of information to enable a mum to breastfeed successfully. It’s through no fault of the healthcare professional, but rather the fault of how their initial training and ongoing training is structured. Therefore their advice and support might often based on personal experiences and/or out of date practices. Not only that but our healthcare professionals also have to work in line with their own NHS trust policies. These differ between trusts and are based not only on NICE guidelines but also considerations such as the skill set of staff and trust finances.
Breastfeeding rates are dropping off drastically after birth
The issue with all this? Published in November 2012, the 2010 Infant Feeding Survey showed that the initial breastfeeding rate in the U.K. was 81%. Across the UK, at three months, the number of mothers breastfeeding exclusively was 17% and at four months, it was 12% (Infant Feeding Survey 2010). However, exclusive breastfeeding at six months is only around 1%. But with the infant feeding survey being cancelled last year and lack of any national leadership or strategy in infant feeding, what hope do we have to improve these figures? What hope do we have of changing the way our health professionals are trained and how their on-going training is structured?
Some people might ask what’s wrong with these figures presented above. In doing so, they reflect a society, our society, in which formula feeding has become normalised. Where friends and family see formula as “just as good” as breastmilk and don’t have their own personal experiences of breastfeeding in order to support new mothers. The World Health Organisation recommends exclusive breastfeeding up to 6 months of age, with continued breastfeeding along with appropriate complementary foods up to two years of age or beyond. It is not within the scope of this post to explore the reasons behind this recommendation, more this article is to raise the issue that breastfeeding families have a dwindling pool of resources from which to obtain support during their breastfeeding journeys. Breastfeeding families are unlikely to be able to rely on advice from healthcare professionals, friends or family. That’s a lonely existence.
How can we change society and health care for new mothers and babies?
All is not lost though. The Unicef Baby Friendly Initiative, launched in the U.K. in 1995 (Unicef UK Baby Friendly Initiative 1995), is based on a global accreditation programme of UNICEF and the World Health Organisation. It is designed to support breastfeeding and parent infant relationships by working with public services to improve standards of care. Maternity units and community facilities have the option to become Baby Friendly accredited and in order to do so are required to provide training for its midwives and health visitors. While the majority of maternity units (91%) and health-visiting services (83%) have achieved or are working towards Baby Friendly status, the remainder have not commenced the process. Therefore new breastfeeding mums can hope that the situation is improving and healthcare professionals that have undergone Baby Friendly training will start to provide the trusted information that mums deserve. But this will require quite a culture shift change within the NHS and this will take time.
There is also lots to be done with the image of, and marketing of infant milk so that “normal infant feeding” moves away from formula and focusses on breastfeeding.
Our society needs educating and this will also need the support and investment from the government.
Kate Butler is a Secondary School Biology teacher by day and mother to two boys (aged 1 and 3) day and night. She trained as a breastfeeding peer supporter in 2013 and since then has set up local peer support meetings in her local area and joined the committee of West Herts Breastfeeders to support with fundraising and event management. West Herts Breastfeeders is a community based mum to mum peer support group that supports breastfeeding families with their breastfeeding journeys in the community and within West Hertfordshire Hospitals NHS Trust. This post was first published on Kate’s blog, The Instinctive Parent (www.theinstictiveparent.org), which she started to share knowledge and help further educate parents to help them make properly informed decisions and choices in how they choose to parent.
WBTi UK Report 2016 – Key findings and what you can do to help
Breastfeeding matters for mums, babies and society.
The WBTi report for the UK shows key gaps and recommendations for improvement in how all of society — the UK Government, national assemblies, local commissioners, friends, family and community — needs to support mothers who want to breastfeed and the healthcare professionals who help them.
In order for this to happen, we need MPs to be aware of the report and recommendations, so that they carry the message to Parliament, and start the change so desperately needed.
MPs are there to listen to your concerns and to represent you in Parliament. Our video explains what the key messages are from the WBTi 2016 Report on the UK, and what we can all do together to make changes happen.
We need YOUR help now in this social media campaign with our video. You can;
Take the report and its recommendations to your local MP
Tag a friend on our Facebook video launch post, like and share the post
Write to your MP or make an appointment to meet them
Post a selfie on our video launch post with the hashtags #breastfeedingmatters and #bfaction to raise awareness on social media and help us make this change
If you have breastfed your own children, if you had hoped to breastfeed but didn’t get enough support, or if you are a health care professional or volunteer supporting breastfeeding women, please get involved.
Mothers have been boldly calling for change, change in the support they need to breastfeed their babies, change in the conversation around breastfeeding. Fathers, partners, health professionals and volunteers have been boldly speaking up in support.
2016 and 2017 has seen lots of activity in the “breastfeeding world”; not that this is a mythical place where breastfeeding is seen as the norm. It’s a real place, just sadly a relatively small world at the moment. We’ve seen a new books on the subject published, we’ve seen campaigns launched, groundbreaking research and reports published, adverts made and most recently a new Bill proposed in Parliament. Any why so much action? Because breastfeeding should be the norm – I’ll go all Biology teacher here and state the obvious – we’re mammals, we have mammary glands in order to be able to feed our young. The breastfeeding world should be everyone’s world.
In recognition of International Women’s Day today, now is the time to #BeBoldForChange (International Women’s Day 2017). Everyone should know about breastfeeding, everyone should feel happy to talk about it, and everyone should feel properly supported about how they choose to feed their baby.
8 out of 10 women stop breastfeeding before they want to (McAndrew et al 2012). There are many reasons for this but Unicef only last week highlighted yet more research showing that breastfeeding support can increase the duration and exclusivity of (Unicef 2017). The World Breastfeeding Trend Initiative UK report (WBTi UK 2016) published in November last year reinforced these findings by identifying a key gap with many mothers lacking access to skilled breastfeeding support. So if mothers aren’t getting support from skilled and trained volunteers or professionals, where is their support coming from?
The current reality is that we live in a society with a formula feeding culture. What does that mean? It means our society sees formula feeding as normal, “just as good” as breastmilk. This is further entrenched in our minds through the media, online, in papers, on television. Families just don’t get the opportunity to make fully informed decisions about how they wish to feed their child because expectations and methods of infant feeding are so ingrained in our culture. “Helpful” friends and family want to support a family’s choice in how they choose to feed their baby but often they have not breastfed so advice can often undermine a family’s breastfeeding journey. Our formula feeding culture is not through the fault of any individual mother or indeed individual healthcare professionals. It’s the result of government not listening to society’s needs; it’s the fault of unscrupulous formula and bottle companies with some pretty amazing marketing strategies. I used to work in marketing – these formula campaigns are ruthless! The Politics of Breastfeeding (Palmer 2009) and Breastfeeding Uncovered (Brown 2016) are fabulous reads if you want to delve further into the impact of politics and commercial interests on breastfeeding.
So what change do we need? On International Women’s Day?
Fundamentally we all – families, supporters, employers, health professionals, politicians – we need to listen to the woman’s voice, the mother’s voice. The mother asking for support and the mothers who can offer the support. We need to celebrate the voices and the hard won wisdom of mothers who have had successful breastfeeding journeys, who have managed to overcome the many challenges they faced. Families who plan to breastfeed need to know what is normal. Many breastfeeding mums ARE happy to talk about their experiences and support and help other mums. But many shy away for fear of stimulating the breast vs. formula debate, the “mummy wars” that are so often fuelled by both the strong feelings of mothers who have been let down, and the deep pockets of the baby feeding industry. Very often the mums who formula feed have done so because they’ve been let down by gaps in the support around them. As mentioned before 8 out of ten women give up breastfeeding before they are ready to and many are not happy about it; this can even lead to an increased risk of postnatal depression (Borra et al; Brown et al). It’s not their fault but the guilt can lead to defensive conversations about how they feed their baby. It therefore shuts down the conversation around breastfeeding and we’re back to square one. These issues are what inspired UNICEF’s ongoing #changetheconversation campaign launched last year (Unicef Baby Friendly Initiative 2016).
Social media is full of private groups where breastfeeding mums have a “safe” place to share and support each other in their breastfeeding journeys without fear of upsetting mums who are not breastfeeding. But why should this be done in private? Why shouldn’t breastfeeding mums shout from the roof tops? It’s great to see that the government’s Start4Life campaign have recently requested to hear from breastfeeding mothers about their stories (Start4Life 2017). It’s a small step but one that may prove powerful. What we really need is to educate our children and our society on breastfeeding. I’m not just saying this because I’m a teacher, but if our children don’t know about it, what hope have we got to normalise it? Breastfeeding families also hold a special role, not shying away from sharing their experiences, but being bold for change and sharing what’s normal in the hope that we can normalise breastfeeding and make our “small” breastfeeding world everyone’s world.
Let’s celebrate the strength of mothers everywhere.
#BeBoldForChange
References
Borra C, M Iacovou and Q Sevilla 2014 New Evidence on Breastfeeding and Postpartum Depression: The Importance of Understanding Women’s Intentions Matern Child Health J DOI 10.1007/s10995-014-1591-z
Brown A, J Rance and P Bennett 2016 Understanding the relationship between breastfeeding and postnatal depression: the role of pain and physical difficulties. Journal of Advanced Nursing Volume 72 (2):273–282 DOI: 10.1111/jan.12832 [Accessed 6/3/2017]
Brown, A. (2016) Breastfeeding Uncovered, Pinter & Martin Ltd 2016













 Kate Butler is a Secondary School Biology teacher by day and mother to two boys (aged 1 and 3) day and night. She trained as a breastfeeding peer supporter in 2013 and since then has set up local peer support meetings in her local area and joined the committee of West Herts Breastfeeders to support with fundraising and event management. West Herts Breastfeeders is a community based mum to mum peer support group that supports breastfeeding families with their breastfeeding journeys in the community and within West Hertfordshire Hospitals NHS Trust. This post was first published on Kate’s blog, The Instinctive Parent (www.theinstictiveparent.org), which she started to share knowledge and help further educate parents to help them make properly informed decisions and choices in how they choose to parent.
Kate Butler is a Secondary School Biology teacher by day and mother to two boys (aged 1 and 3) day and night. She trained as a breastfeeding peer supporter in 2013 and since then has set up local peer support meetings in her local area and joined the committee of West Herts Breastfeeders to support with fundraising and event management. West Herts Breastfeeders is a community based mum to mum peer support group that supports breastfeeding families with their breastfeeding journeys in the community and within West Hertfordshire Hospitals NHS Trust. This post was first published on Kate’s blog, The Instinctive Parent (www.theinstictiveparent.org), which she started to share knowledge and help further educate parents to help them make properly informed decisions and choices in how they choose to parent.

