A network of trained peer support is an essential part of high quality integrated breastfeeding services.
Unicef UK Baby Friendly Initiative (BFI) outlines three components that good local breastfeeding services must include, in order to be awarded Baby Friendly accredited status.
Basic, or Routine Care
All health workers who work with new families (health visitors and any allied healthcare assistants in the community services) have been trained to BFI standard (approximately 18 hours of initial in service training, with yearly updates of an hour or more).
Additional services
Here BFI outlines how every health visiting and community service must be embedded in and well supported by a network of trained peer supporters, or other social and trained breastfeeding support. NICE recommends that peer support programmes be externally accredited. Good practice includes not only training, but also regular supervision and updates of skills and knowledge. Typical peer support programmes require peer supporters to be experienced breastfeeding mothers, and often expects them to come from similar communities as the population they are supporting. Training generally is part time, over 16-36 hours. Peer supporters work in a supervised setting, acting as an “informed friend,” and referring complex cases on to health professionals or an advanced breastfeeding practitioner such as an IBCLC or breastfeeding counsellor, using a referral pathway.
Breastfeeding counsellors in the UK are also experienced breastfeeding mothers, so they also provide a type of peer support, or “mother-to-mother” support. Their training typically take around two years, and they are autonomous practitioners, who can be responsible for leading their own local breastfeeding support groups, usually through one of the main UK breastfeeding voluntary organisations.
Mothers who are experiencing breastfeeding challenges often need more than one visit – and they need the time that it requires for skilled listening as well as exploration of possible breastfeeding strategies to resolve the issue. Although many health visitors have additional breastfeeding training and skills, the health visitor workforce is vastly overstretched, and it simply isn’t possible to provide the time and the number of visits that many breastfeeding mothers need.
But peer support programmes can provide this – they offer groups where lonely mothers can meet others and gain confidence in their own mothering, alongside skilled listening and well- informed support. Many mothers will find their own “village” in their local breastfeeding support group, and will return again and again. Some will go on to train as peer supporters or breastfeeding counsellors themselves.
Peer support groups are the beating heart of breastfeeding support
Helen Gray, WBTi Joint Coordinator
WBTi audit of peer support and breastfeeding counsellors provided by the voluntary sector, 2016 In Part 2 of our WBTi UK Report
Specialist support
Every area should have a referral pathway to specialist care at the IBCLC (International Board Certified Lactation Consultant) or similar level, for those complex cases where breastfeeding issues cannot be resolved at the level of basic/ routine care or by additional peer support.
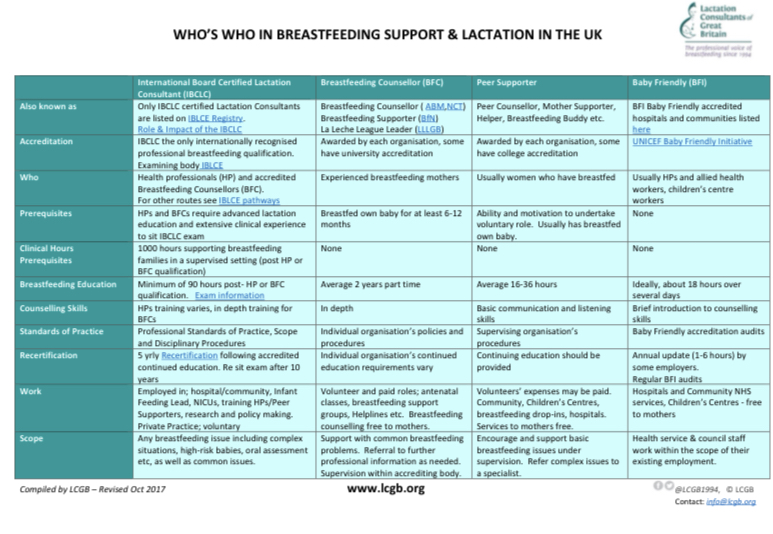
The different roles of breastfeeding support in the UK have been outlined in the chart below:
WBTi’s research: Case studies of best practice The WBTi 2016 Report featured several case studies of areas who showed best practice in providing well joined up, integrated breastfeeding services: Brighton and Harrow.
More recently, our WBTi team has presented posters featuring these and additional case studies of best practices in providing integrated breastfeeding services: Medway, Harrow and Swindon.
WBTi Poster on Integrated Breastfeeding Services.
These examples of best practice in integrated breastfeeding services gave concrete results.
They demonstrated:
– a 2% rise in breastfeeding rates in a socially deprived area in 2018 (Medway),
– a 15% rise in initiation and a 12% rise in continuation of breastfeeding over a six year period (Harrow)
– and a 6% reduction in drop off rates from birth to 6-8 weeks over six years (Swindon).
Our WBTi team are always on the lookout for further examples of best practice in integrated breastfeeding services, and we submit them to Public Health England. Please do contact us if you would like to submit your local services!
Helen Gray MPhil IBCLC is Joint Coordinator of the World Breastfeeding Trends (WBTi) UK Working Group. She is also an accredited Leader (breastfeeding counsellor) with La Leche League of Great Britain.
For Day 2 of WBW we are very pleased to have a guest blog by Health Visitor and Clinical Research Fellow Dr. Sharin Baldwin.
Breast milk provides the ideal nutrition for infants and its associated benefits to the infant, mother and the wider public health are well documented. Traditionally breastfeeding promotion and advice have been targeted at expectant and new mothers, with an aim to increasing breastfeeding rates in infants. In recent years it has been acknowledged that partners play an important role in supporting women’s decision to breastfeed, while also providing practical and emotional support with the continuation of breastfeeding. Research highlights the important role of fathers in promoting and supporting their partners with breastfeeding (Tohotoa et al., 2011; Datta et al., 2012; Sherriff et al., 2014; Hansen et al., 2018), but in practice fathers continue to report inadequate levels of information and support from health professionals. Training for health professionals therefore should consider men’s needs relating to breastfeeding promotion and support, as well as women’s.
New fathers have often reported finding their partner’s breastfeeding experiences to be much more difficult than they had originally anticipated, with many not knowing how to help or support their partner with breastfeeding when they experienced difficulties (Baldwin et al, 2018; 2019). This is where health professionals can really make a difference. They can help educate and prepare expectant fathers better during the antenatal period by providing them with ‘realistic’ information about the time it may take for their partner to establish breastfeeding. It is also important to highlight some of the breastfeeding challenges they may face in early parenthood and what strategies or support are available to overcome them. This will help men to develop more realistic expectations of the processes involved with establishing breastfeeding and make them feel more empowered to support their partner when faced with any difficulties.
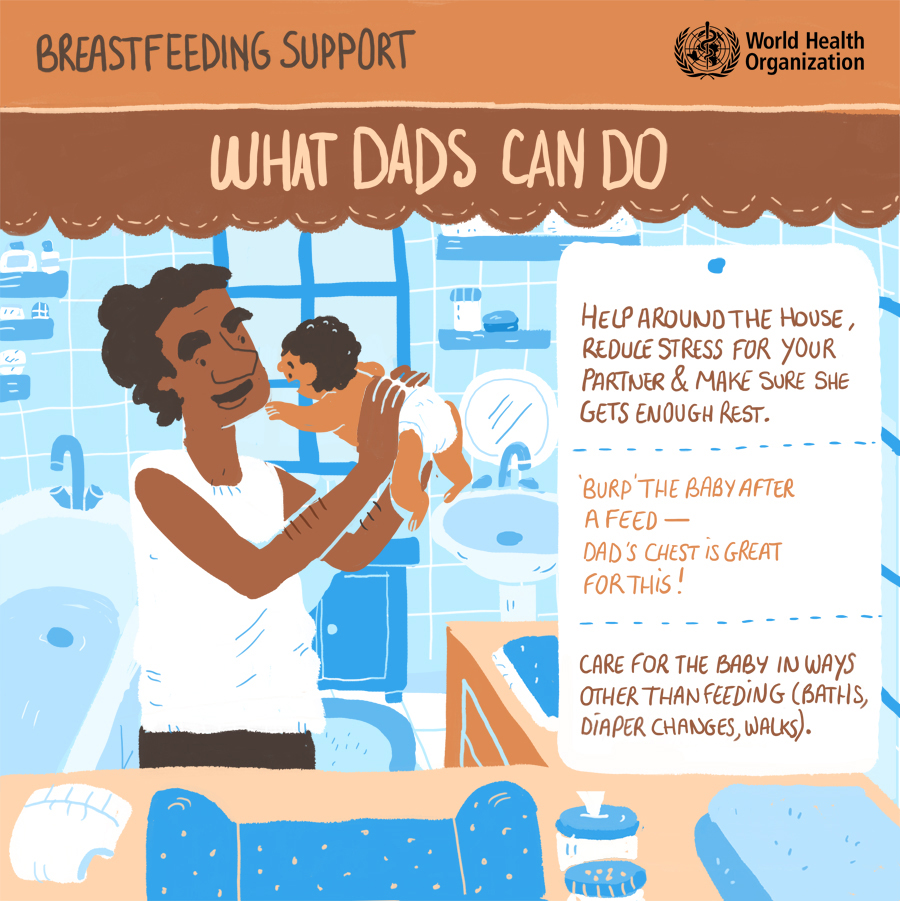
While fathers may not be able to be directly breastfeed their babies, they need to know that they play a crucial role in making breastfeeding a success. They can provide practical support to their partners through helping with household duties, giving them a massage, allowing them to rest, making meals and drinks for them, and giving them emotional support through regular praise, reassurance and encouragement. Good levels of breastfeeding support are likely to make the process easier and more enjoyable, while giving women the confidence to continue breastfeeding for longer. Fathers’ involvement in breastfeeding not only has the potential to increase breastfeeding rates and duration, but also contribute to better outcomes for babies, mothers and the wider public health agenda. So, let’s not forget about including fathers when having those crucial discussions and training about breastfeeding!
Baldwin, S., Malone, M., Sandall, J., Bick, D. (2018) Mental health and wellbeing during the transition to fatherhood: a systematic review of first-time fathers’ experiences. JBI Database of Systematic Reviews and Implementation reports, 16(11):2118–91.
Baldwin, S., Malone, M., Sandall, J., Bick, D. (2019) A qualitative exploratory study of UK first-time fathers’ experiences, mental health and wellbeing needs during their transition to fatherhood. BMJ Open 2019;9:e030792. doi:10.1136/bmjopen-2019-030792 https://bmjopen.bmj.com/content/9/9/e030792.info
Datta, J., Graham, B., Wellings, K. (2012) The role of fathers in breastfeeding: decision-making and support. British Journal of Midwifery, 20(3):159–167.
Hansen, E., Tesch, L., Ayton, J. (2018) ‘They’re born to get breastfed’- how fathers view breastfeeding: a mixed method study. BMC Pregnancy and Childbirth, 18:238 https://doi.org/10.1186/s12884-018-1827-9
Sherriff, N., Hall, V., Panton, C. (2014) Engaging and supporting fathers to promote breast feeding: A concept analysis. Midwifery, 30: 667–677.
Tohotoa, J., Maycock, B., Hauck, Y.L., Howat, P., Burns, S., Binns, C.W. (2009) Dads make a difference: an exploratory study of paternal support for breastfeeding in Perth, Western Australia. International Breastfeeding Journal, 4: 15. http://dx.doi.org/10.1186/1746-4358-4-15
Author:
Dr. Sharin Baldwin PhD, MSc, PG Dip, BSc (Hons), HV, RM, RN, QN, FiHV, IHV Research & PIMH Champion
NIHR Clinical Research Fellow, University of Warwick
Clinical Academic Lead (Nursing and Midwifery), London North West University Healthcare Trust
This may be the end of World Breastfeeding Week 2020 but campaigning for good breastfeeding support to be readily available to all mothers with young babies and for society to value breastfeeding, in order to maximise the population’s health and help protect the environment, continues.
This year Covid-19 lockdown has been an added complication for families, with minimal face-to-face contacts, and we do not know how long restrictions will need to continue. This is your opportunity to let us know what support you think is needed in the months ahead by using the Leave a Reply button below. Reading S’s story may help you identify what’s needed.
S gave birth to her first baby R in January and movingly describes her experiences and how she found the feeding arrangement that worked best in her circumstances:
“So R turned 6 months old last weekend and he is really thriving! I am still breastfeeding him which I am so proud I continued with, and it definitely got easier as time went on. It has always been a combined method with the bottle but his milk intake of breast has always been at least 60-75%. My milk supply never caught up after the mastitis no matter how much expressing and breastfeeding I did, and I found it was also really hard to try and sustain that vigorous cycle with my ME – I started to have really bad days where I just couldn’t function so it was easier for my husband to feed R with expressed milk and top up with formula if necessary. I do feel that the routine we got into with breastfeeding, expressing and bottles was the best we could do in our particular situation and he’s such a healthy little boy. I’m really glad I persevered with it all.
We started baby-led weaning about a fortnight ago and R is loving interacting with all the different foods! He especially loves broccoli (he was so keen on it, that not only was he feeding himself the various stalks I’d put on his tray, but he was trying to lick the tray too to get all the broccoli off!!), avocado, sweet potato, carrot, pear and banana. He wasn’t so keen on mashed potato – he preferred to wear it instead!
Life has been really strange and difficult in lockdown if I’m honest. It’s felt quite lonely, as I’m sure it has for everyone else, but we’ve really struggled at times to keep going without familial or friend support. The extra perinatal support I was having became video calls which I’m really grateful for but isn’t the same as in person. Aside from the difficulties, he’s such a lovely happy boy – I’m so proud!”
Breastfeeding has been shown in many studies to be linked to better health in babies and mothers. As breastfeeding is the physiologically normal way for infants to be fed, it is more accurately stated that not breastfeeding is associated with poorer levels of health. This is not surprising as infant formula only provides the basic nutrition a baby needs (proteins, carbohydrates, fats, minerals and vitamins) but breastmilk is an amazing fluid with over 300 different components, as shown here. It includes growth factors, hormones, enzymes and anti-microbial factors as well as nutrients, and varies in exact composition according to the needs of the baby. It is therefore unique for each mother at each moment in time.
Knowing how amazing human milk is can help a mother have determination to overcome breastfeeding difficulties but it can also feel like pressure. What she needs is access to accurate information and suggestions, offered in a caring way after listening to her particular situation. That means that everyone who has contact with new mothers needs to have sufficient knowledge and person-centred communication skills.
Rachel describes her experiences of giving birth and breastfeeding during lockdown.
Rachel’s story
“During my three years of trying to conceive and infertility treatment I often fantasied about the closeness of holding my baby and feeding them. When I was lucky enough for my IVF to work, I moved on from worrying about if I could have a baby to if I could breastfeed. My mum assured me it was easy for her but her emphasis on its importance felt like further pressure. Many of my friends had stressful experiences and got medical advice that they needed to supplement with formula. Towards the end of my pregnancy I got a phone call from the hospital to explain all the benefits of breastfeeding and recommended I harvest colostrum at 37 weeks. I tried this but couldn’t get even a drop which further made me doubt my ability to breastfeed.
My baby was born in May during the pandemic, so I wasn’t allowed a water birth and my husband was only allowed in during active labour. This meant when I was 3 cm dilated and having intense contractions he had to wait outside the hospital in the car. They refused to check my dilation again for five hours due to infection risk and left me alone. When around 4 hours later I felt the urge to push I convinced the midwife to stay and help. When they could see my baby’s head, I was allowed to telephone my husband and ask him to come. My husband was there for the last 10 minutes but it had been a lonely labour due to COVID-19 without most of the plans I had made that involved a birthing partner.
After the birth the level of support dramatically increased with my husband and midwives all keen to help. My baby was placed on my chest and knew instinctively how to feed and stayed on for hours, it was amazing. I continued to use the gas and air for this first feed as for me the breastfeeding gave me very strong period-like contractions. After this first feed, I no longer had the period-like contractions, but my nipple started to become sore. I decided to stay a night in the hospital for some extra breastfeeding and baby care support, as most face-to-face community support wasn’t available at that time. The midwives repeatedly showed me how to improve my breastfeeding latch throughout the night.
The first breastfeed
Five days after the birth I saw the doctor for routine checks. The doctor calculated my baby had lost 7% of her baby weight (which I believe is normal) but she still asked if I was feeding my baby enough. She asked if my breasts were soft and empty after feeding. At this point my milk hadn’t come in so I didn’t understand the doctor even when I asked her to explain more and had to say no they don’t empty. She also had a look at my nipples and said they were cracked so insisted I must use a nipple shield and wouldn’t discuss any other options. After the appointment I cried in the car park that I couldn’t feed her properly and was failing as a mother. On the way home we rushed to shop for nipple shields (the first shop I had been in since the start of lockdown). I couldn’t get the shields to work and my internet research in some cases strongly warned against their use. I didn’t know what to do so rang my mum and then the hospital. I spoke to a lovely midwife who reassured me and said I didn’t have to use nipple shields and that my nipples could heal with continued feeding.
Due to COVID-19 I had a triage phone call with the health visitor the following week, to assess if I needed a visit. She decided that I needed a visit to weigh my baby and gave me leaflets about local breastfeeding support as my nipples were still painful during feeding. There was no face-to-face support available, but I had a video call with the breastfeeding advice line and joined a virtual group. These calls have been great for giving me personalised support to improve my breastfeeding latch so that feeding is no longer painful, listen to my concerns and build my confidence. It is also very convenient as I don’t need to leave my home for it.
My baby is now almost 10 weeks old and breastfeeding is going well. I can feed her watching TV, half asleep in the dark or on the bench in the park without much effort and with no discomfort. I am also pleased not to need to warm up formula as that might be harder when cafes and other facilities are closed due to COVID-19. I love being close to my baby during breastfeeding and being able to provide what she needs.”
Thank you very much, Rachel, for sharing your story.
As part of World Breastfeeding Week, #WBW2020 and #GreenFeeding, we’re emphasising the importance of mothers having easy access to good quality breastfeeding support, if and when they need it. This is partly provided by skilled people and partly by evidence-based written information.
This short leaflet for new parents gives tips about breastfeeding during the pandemic and also lists reliable sources of information and support. The aim is to help empower families who may be much more isolated than families generally were before the Covid-19 pandemic and have limited access to face to face help from health professionals and local breastfeeding support groups.
A slightly shortened two-page landscape version of the leaflet can be downloaded from here.
How do I manage as a new mother breastfeeding during the Covid-19 pandemic?
How can I best protect my baby?
Breastfeeding is one of the most important ways you can protect your baby. Your body makes antibodies in your milk which help your baby fight infections. Breastfeeding also helps babies develop a good long term immune system, and also help to protect mothers from breast cancer, heart disease, obesity and diabetes.
No evidence has been found that coronavirus is passed through breastmilk. Mothers make specific antibodies to any infections they are exposed to, and these pass into their milk. This means that a mother with Covid-19 can help protect her baby against all kinds of pathogens by breastfeeding, and may even provide specific antibodies to the novel coronavirus.
Covid-19 precautions
However a baby is fed, they could be exposed to Covid-19 if their carer coughs or sneezes over them so the parent/carer might prefer to wear a face covering when in close contact and needs to wash their hands regularly. RCOG (the Royal College of Obstetricians and Gynaecologists) provides more details under Advice for women with suspected or confirmed coronavirus infection who have recently given birth.
Fewer visits to GP or hospital
Exclusive breastfeeding for 6 months, then continuing to breastfeed alongside other foods, helps babies to be as healthy as possible and lowers their chance of needing to see a GP or have a hospital stay, e.g. for ear or chest infections.
Food security
Breastfeeding means parents do not have to worry about formula supplies or even shop for formula.
How do I know my baby is getting enough?
Babies are normally weighed at birth, 5 days & 10-14 days (when the health visitor usually takes over from the midwife). With the pandemic, there may be few opportunities to have your baby weighed or see your midwife or health visitor face-to-face.
However, your baby’s behaviour and nappy contents can help you know if your baby is getting enough milk.
The first 6 days are a time of change. From mid-pregnancy breasts produce a thick, usually yellow, type of milk called colostrum. A few days after birth, colostrum transition to more mature milk. The breasts usually feel very full at this time. The poos change too:
thick black meconium for the first couple of days after birth
green around Day 3 to 4
At least two yellow poos each day, by Day 5 to 6
A baby who is getting enough shows this pattern, takes themselves off the breast and generally settles after feeds. For photos of nappy contents see this NCT information.
From 6 days to around 6 weeks, milk intake is probably fine if:
your baby is usually contented after feeds
has at least 6 heavy wet nappies/ day
has 2 poos each at least the size of a £2 coin per day
After 6 weeks, some babies poo less often but the overall amount is about the same.
In the first two weeks, if your baby hasn’t pooed for 24 hours, contact your midwife and a breastfeeding helpline or local supporter for help.
How do I know breastfeeding is going well?
It’s going well if your baby is getting enough and you are finding breastfeeding comfortable.
Start4Life provides very useful information about how breastfeeding helps the health of babies and mothers and how to help your baby latch on well.
However, if your baby often falls asleep during feeds and wakes up again hungry after a few minutes, feeds are regularly longer than an hour, or it is uncomfortable or painful for you, the most likely reason is that your baby isn’t latched well enough to feed effectively.
How can I increase my milk supply?
If your baby is producing less wee and poo than expected, or you are topping up with formula,
can you breastfeed more often – another feed or two in 24 hours?
are you offering both breasts at every feed? you could switch back and forth during a feed
breast compression can increase milk flow
can you contact a helpline or breastfeeding supporter for more suggestions?
Remember – if you feel your baby is feeding very often, they are trying to get enough milk, and also helping to increase your milk supply.
And if breastfeeding isn’t going well?
To latch well the baby needs to gape wide, have the nipple in the upper part of their mouth, and chin pressed against the breast. Snuggle your baby close, head free, nose level with your nipple. This detailed information from La Leche League shows different positions you could try, and ways of helping your baby latch better.
If feeding is painful, or you are breastfeeding very frequently but your baby isn’t getting enough milk, get skilled help! You can also express your milk and offer your baby expressed milk until your baby starts feeding better and your nipples have healed. The Breastfeeding Network has information about expressing and storing breastmilk. Your midwife or health visitor can help you learn to use a cup or bottle safely.
Where can I get skilled help?
You can contact the local midwifery team or health visiting service using the phone numbers you’ve been given. Often there is an Infant Feeding Coordinator or team who can provide more specialised support. They may also put you in contact with a volunteer breastfeeding counsellor or peer supporter. There are several charities continuing to offer free skilled breastfeeding support (see below). Your GP is the appropriate contact for medical situations – such as mastitis that isn’t improving after 24-48 hours – alongside breastfeeding support.
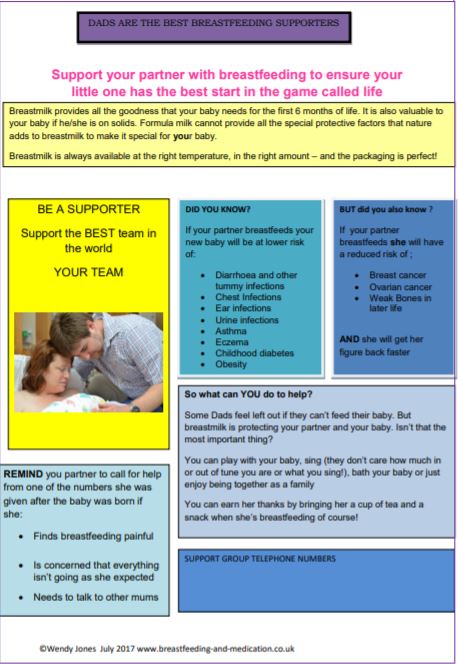
Partners and family support
Her partner can be a huge support to a mother who is breastfeeding and one possible silver lining of the pandemic is that many are at home and able to give more support.
UK breastfeeding helplines
National Breastfeeding Helpline 9.30am – 9.30 pm
0300 100 021
La Leche League GB (LLLGB) (web chat and email also available)
0345 120 2918
La Leche League Northern Ireland
028 95 818118
NCT Helpline 8am – 12 midnight
0300 330 0700
Breastfeeding Helpline for Bengali/Sylheti speakers
0300 456 2421
Breastfeeding Helpline for Tamil/Telugu/Hindi speakers
NCT – details of free local Zoom support groups available via the helpline: 0300 330 0700
IBCLCs (International Board-Certified Lactation Consultants) – these may work for the NHS, voluntarily or provide a paid-for service. To find an IBCLC see the LCGB website.https://www.lcgb.org/find-an-ibclc/
Further information and self-help suggestions for common concerns listed below are described on several websites, such as the Institute of Health Visiting Parent tips, NCT’s information on breasts after birth and the NHS website.
My breasts are hard and painful
In the early days, this could be engorgement. Frequent feeding helps. La Leche League provides detailed information.
I have a small tender area in one (or both) breasts
This could be a blocked duct. Gentle massage over the area while feeding often helps.
I feel fluey and have a hot, hard, red area on my breast
This is likely to be mastitis. Removing milk, by feeding baby or by expressing, is the most helpful action, along with other self-help measures described here. La Leche League provides detailed information.
I think my baby has tongue-tie
A tongue-tie only needs to be divided if it is significantly affecting feeding. If breastfeeding is affected, the first step is to check the baby is as well-latched as possible. For families who may have to wait for treatment during COVID19, this is a very useful and detailed article by Sarah Oakley, IBCLC.
My baby takes a lot when I bottle feed
“I’m giving some top-ups for the moment because my baby lost too much weight but he takes a lot quickly and then is uncomfortable with wind.” Having the bottle level rather than tilted and giving the baby pauses helps the baby cope with the flow from a bottle and it can be easier to tell when the baby has had just enough. This is called ‘responsive bottle feeding‘.
My mother-in-law keeps wanting to give my baby formula
ABM (the Association of Breastfeeding Mothers) has a leaflet for grandparents to help them understand what is now known about breastfeeding.
I stopped breastfeeding but now I want to restart
This can be done but needs commitment as it takes a while to build up the milk supply again. You may find it easier if you have someone providing you with ongoing skilled support with relactation.
Our message to you
We hope the above information, and support options if you need them, can help towards you enjoying breastfeeding and continuing for as long as you and your baby want to.
Authors: The WBTi UK Steering Group – Helen Gray, Clare Meynell, Alison Spiro, Patricia Wise; design by Carol Smyth
New Unicef Baby Friendly learning outcomes for health professional training
It had been announced at the Baby Friendly conference in 2018 that learning outcomes and resources were being produced.
Addressing gaps
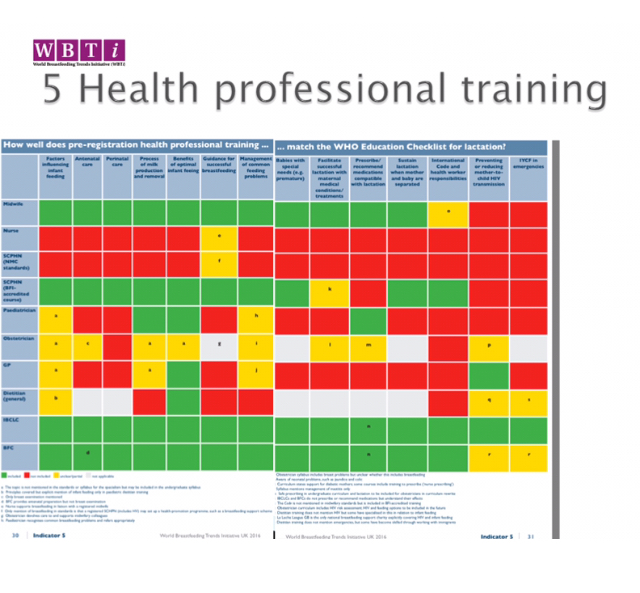
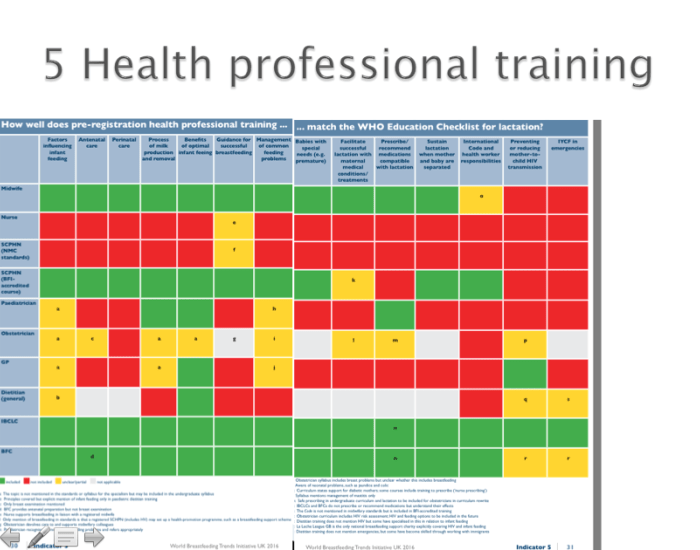
WBTi UK Indicator 5: Health professional training
The WBTi report in 2016 (see Indicator 5 in Part 1 of the WBTi UK report for the above table, and Indicator 5 in Part 2 for the detailed findings for each UK health profession) showed that for most health professions in the UK, the coverage of infant feeding in pre-registration training was inadequate. In some case only broad standards are given and the individual universities develop their own curricula.
The infant feeding learning outcomes launched by BFI are for a range of newly qualified health professionals so they ‘articulate the minimum knowledge and understanding of infant feeding that it would be reasonable to expect from a health practitioner at the point of qualification’. There are slightly different ones for the following five groups:
doctors
dietitians
pharmacists
children’s nurses
maternity support workers/nursery nurses.
For each of these professional groups the learning outcomes are grouped into three broad themes:
The value of human milk and breastfeeding.
Supporting infant feeding.
Infant feeding in context, which includes understanding the importance of the International Code.
They are intended as ‘a stimulus to universities and others to start to consider what should be covered in relevant curricula and training, and then to take action to make that a reality.’
One useful recommendation is that ‘A mapping exercise can help the university to assess how far the topics are already covered and assessed in the curriculum, and to identify and plan for any additions to modules or design alternations needed.’ Plans for the resources ‘include a slide pack to help lecturers deliver the content to students, e-learning for students and assessment examples’.
Specific learning outcomes like these, provided they are taken on board by the training institutions, will surely help to achieve a higher and consistent level of knowledge and skills within and between health professions.
Cover photo licensed by Adobe Stock
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group.
I’m a lactation consultant and writer who has just finished a Masters degree in Health Promotion at Leeds-Beckett University. This blog touches on some of the insights that my studies have given me, not least how data, like WBTi’s reports, can help health promoters create integrated, sustainable solutions that make health a resource to be shared by everyone.
In 1986, the World Health Organization (WHO) Ottawa Charter for Health Promotion defined Health Promotion as “the process of enabling people to increase control over, and to improve, their health.” Whether the focus be on breastfeeding, preventing obesity, supporting mental health or any of the complex (so called ‘wicked’) problems that challenge our societies, it is health promotion’s recognition of the social determinants of health that has most affected my thinking. All too often our society is quick to blame the individual for unhealthy behaviours; my increased awareness of the social determinants of health, that is, how socio-economic, cultural and environmental conditions determine individuals’ well-being, has changed my perception. It’s given me a heightened awareness of how prevailing political ideologies influence the way we think about society, and how this plays out into how likely (or not) individuals are to be able to make healthy choices throughout the course of their lives.
“This unequal distribution of health-damaging experiences is not in any sense a ‘natural’ phenomenon but is the result of a toxic combination of poor social policies, unfair economic arrangements …and bad politics.” WHO[1]
To give an example, indicator 6 of the WBTi looks at community-based support, so key to women continuing to breastfeed.[2]In the UK, the recent NHS Long Term Plan’s recommendation of UNICEF UK Baby Friendly accreditation is cause for celebration and will boost the capacity of midwives and health visitors to support breastfeeding in the community.
However, cuts to peer-support services, and the closure of over 1000 Sure Start centres have disproportionately affected poorer members of society. If a mother in the community has persistent nipple pain, no car, no public transport, no money for a lactation consultant and her nearest breastfeeding group is 20 miles away, even with the support of the hard-working volunteers on the National Breastfeeding Helpline, her capacity to protect the health of her family through breastfeeding will be limited.
Incidentally, the discipline of Health Promotion, while focusing on the up-stream causes of health inequalities, is also focused on empowering communities to participate in the creation of healthier societies. The UK’s WBTi report, under Indicator 6, points out that in England and Wales there is often little coordination between NHS services and peer-supporters, who can offer so much to new mothers. It recommends a range of integrated postnatal services that include voluntary sector breastfeeding support, meet local needs and provide clear access to specialist support.
Integrated breastfeeding support is outlined in the criteria for UNICEF Baby Friendly accreditation for community services:
Basic: universal services such as midwives, health visitors, and support workers are trained to BFI standards
Additional: a network of trained local peer supporters and support groups
Specialist: a referral pathway to specialist help at IBCLC level, for complex cases that cant be resolved by “Basic” and “Additional” support
As an individual health promoter, the scale and complexity of the social determinants of health can feel overwhelming. Nonetheless, recognising them sets the challenge to health promoters (in all disciplines, not just those who work in traditional health services or policy) to work empathetically, creatively and collaboratively. After all, ‘Success in breastfeeding is not the sole responsibility of a woman – the promotion of breastfeeding is a collective societal responsibility’ (The Lancet).
Alice Allan is a lactation consultant, writer and communication specialist who has worked in Ethiopia and Uzbekistan on maternal and child health. Her novel, Open My Eyes, (Pinter and Martin) set in an Addis Ababa NICU, recently won The People’s book Prize for Fiction. She currently lives near London with her family and an Ethiopian street dog called Frank.
During World Breastfeeding Week #WBW2019, we are hosting a series of guest blogs exploring how the wider team of health professionals and community breastfeeding support can support breastfeeding families. The WBTi Report found numerous gaps in health professional training in infant feeding, and we are delighted to see a terrific range of resources being developed to address this.
In this blog, Wendy Jones MBE discusses gaps in the training of pharmacists (See Indicator 5 in Part 2 of the WBTi report for our detailed findings on pharmacist training) and introduces her new free online educational resources for pharmacists.
On a daily basis I hear that pharmacy staff have advised mothers not to breastfeed whilst taking medication or have refused to sell products such as antihistamines to lactating mothers. This is frustrating for families (and me!) and unnecessary.
We know that there are barriers around breastfeeding and medication:
The patient information leaflet – invariably it says that the product should not be used during lactation. This doesn’t imply risk usually rather that the manufacturer didn’t include breastfeeding when applying for marketing authorisation. For more information see this leaflet on the Breastfeeding Network website.
Understanding of the importance of breastfeeding for the future health of mother and child. Sadly breastfeeding, let alone understanding the pharmacokinetics of transfer of drugs into breastmilk, is not covered currently in most undergraduate training. Most knowledge relies on personal experience (Jones W 2000 Doctoral thesis University of Portsmouth. The role of community pharmacy is supporting mothers requiring medication).
Fear of litigation – to sell a medicine outside of its licence application entails taking responsibility. Pharmacists are concerned, rightly so if they do not access evidence-based information (Hale TW Medications and Mother’s Milk, Jones W Breastfeeding and Medication, LactMed , UKDILAS, Breastfeeding Network factsheets)
Time – frequently counter assistants rather than busy pharmacists are involved in sales of simple medications and do not discuss safety in breastfeeding unless asked by the mother.
Time limitations to consult expert sources.
Conflicts of interest
It has come to my attention recently that continued professional development (CPD) materials on infant feeding are being provided free of charge to make pharmacists and staff “Infant Feeding Champion”. Sadly, these are provided by the formula companies and the support of breastfeeding is considerably less than what I would describe as evidence based and full of advertisements for products ranging from nipple shields to nipple creams and specialist formulas.
New free training materials
I decided that I wanted to provide training materials for pharmacists and counter staff free of charge using the knowledge that I have gained over the past 31 years as a qualified, registered breastfeeding supporter as well as pharmacist with a specialist interest in the safety of drugs in breastmilk. The first module can be found here. More modules are underway looking at the pharmacokinetics of drug transfer and the treatment of common conditions.
In the meantime, my message is #DontSayStopLookItUp
I’m happy to be contacted:
by email at: wendy@breastfeeding-and-medication.co.uk
Wendy was one of the founder members of a UK charity the Breastfeeding Network. In her employed life she was a community pharmacist and also worked in doctor surgeries supporting cost effective, evidence-based prescribing. She qualified as a pharmacist prescriber using her knowledge to reduce the risk of heart attacks and strokes in clinics to help patients stop smoking, weight optimisation and control of blood pressure and cholesterol. She feels she was best described as the conscience of the village. Her aim was to run clinics for breastfeeding mums needing medication but never managed it.
Wendy left paid work to concentrate on writing her book Breastfeeding and Medication (Routledge 2013, 2nd edition 2018), developing information and training material on drugs in breastmilk as well as setting up her own website http://www.breastfeeding-and-medication. She has also published Breastfeeding for Dads and Grandmas (Praeclarus Press) and Why Mothers Medication Matters (Pinter and Martin).
Wendy is known to many from her work on providing a service on the compatibility of drugs in breastmilk and has been a breastfeeding supporter for 30 years. She is passionate that breastfeeding should be valued by all and that medication should not be a barrier. She has 3 daughters and 5 grandchildren ranging in age from 6 years to 6 weeks. All her family seem as passionate about breastfeeding as she is and currently all 3 of her daughters are breastfeeding.
She was awarded a Points of Light award by the Prime Minister in May 2018 and was delighted to be nominated for an MBE in the New Year’s Honours List 2018 for services to mothers and babies. She received her award at Windsor Castle in May 2019 from Her Majesty the Queen.
During World Breastfeeding Week #WBW2019, we are hosting a series of guest blogs exploring how the wider team of health professionals and community breastfeeding support can support breastfeeding families. The WBTi Report found numerous gaps in health professional training in infant feeding, and we are delighted to see a terrific range of resources being developed to address this.
As a reminder, the Hospital Infant Feeding Network is a place for hospital health professionals to find out more about facilitating and supporting breastfeeding in a hospital setting. It provides a highly referenced, practical website on relevant topics, and a closed Facebook group for discussion and sharing best practice. For National Breastfeeding Celebration weeks in June, HIFN produced a set of A3 posters aimed at hospital staff in different settings to summarise useful, evidence-based information. These can be downloaded here.
The first two posters look at the reasons for health professionals to support breastfeeding, in term babies and in the neonatal unit setting. Families who are finding breastfeeding difficult are unlikely to find this type of messaging useful so it is important that these are placed to be staff-facing only.
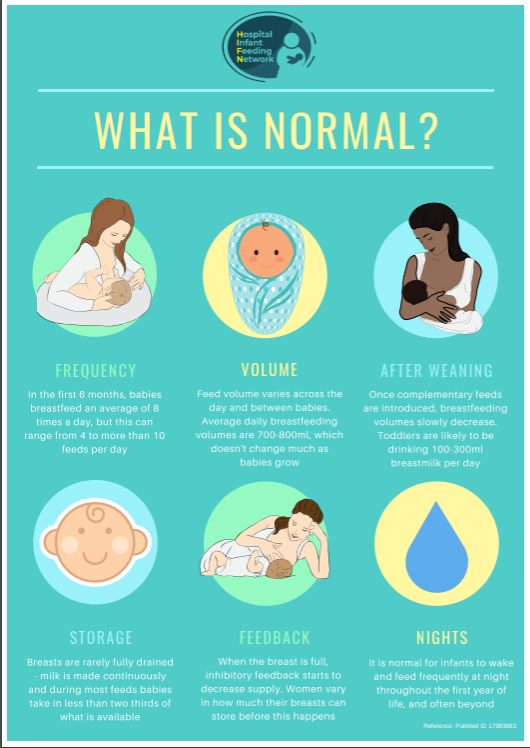
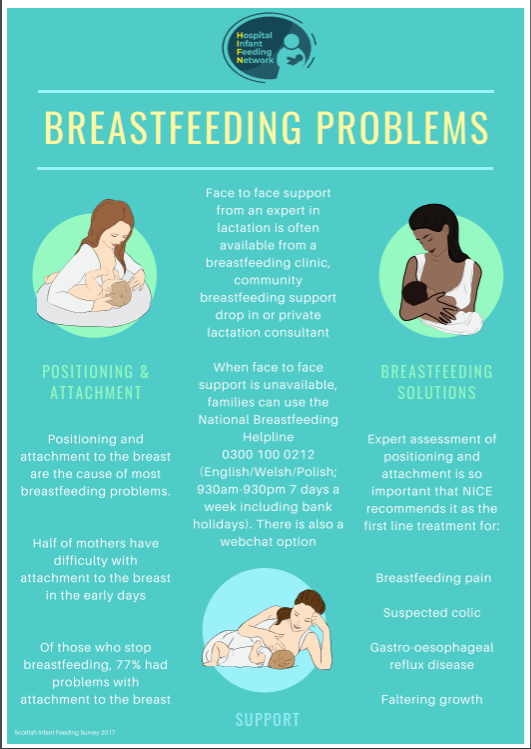
The next three posters look at what is normal, common breastfeeding problems and the non-nutritional aspects of breastfeeding:
The final poster is designed for hospital settings where lactating women might be seen or admitted:
More information about all of these topics is available on the HIFN website.
Ilana Levene is a paediatric doctor planning to sub-specialise in neonatal medicine and interested in research relating to neonatal nutrition. She lives in Oxford with her husband, an environmental consultant, and two children. She is a trustee of Oxfordshire Breastfeeding Support, a local grassroots network of free weekly breastfeeding drop-ins and online support. She likes cross-stitching and making patchwork quilts.
During World Breastfeeding Week #WBW2019, we are hosting a series of guest blogs exploring how the wider team of health professionals and community breastfeeding support can support breastfeeding families. The WBTi Report found numerous gaps in health professional training in infant feeding, and we are delighted to see a terrific range of resources being developed to address this.
This campaign, started by the GP Infant Feeding Network in 2017, aims to make sure healthcare professionals know how to check whether specific medicines can be taken by breastfeeding women. Most healthcare professionals know that with regard to breastfeeding and medication they should check what the British National Formulary (BNF) says. The BNF is a phenomenal resource, respected around the world, with comprehensive information about medication doses, side effects and cautions. However, in some cases it takes a very cautious line on breastfeeding – for example, for the antidepressant sertraline, recommended by specialist services as a preferred option in breastfeeding, the BNF says “not known to be harmful but consider discontinuing breastfeeding”. For ibuprofen, accepted by specialist services as appropriate during lactation, the BNF says “use with caution during breastfeeding. Amount too small to be harmful but some manufacturers advise avoid”. It isn’t hard to see that well-meaning healthcare professionals are nervous about recommending medicines for breastfeeding women when seeing these descriptions in a trusted source of information, and why they may advise that breastfeeding should be stopped, or that the medication cannot be taken.
The #Don’tSayStopLookItUp campaign seeks to highlight the position of the National Institute for Health and Care Excellence (NICE), which states “Ensure health professionals who prescribe drugs to a breastfeeding mother… seek guidance from the UK Drugs in Lactation Advisory Service… the ‘British National Formulary’ should only be used as a guide as it does not contain quantitative data on which to base individual decisions… Health professionals should recognise that there may be adverse health consequences for both mother and baby if the mother does not breastfeed. They should also recognise that it may not be easy for the mother to stop breastfeeding abruptly – and that it is difficult to reverse”. The campaign poster set can be downloaded, and covers common classes of drugs such as antibiotics, antidepressants, painkillers and anaesthetics. The rest of the blog will cover in more detail how health professionals can effectively use the UK Drugs in Lactation Advisory Service (UKDILAS).
UKDILAS is an NHS service specifically set up to help health professionals make informed decisions about the use of medicines during breastfeeding. It is provided by a team of highly specialised pharmacists. The website is not the easiest one to navigate so we’ll go through the three particularly useful services they provide, step by step.
Using UKDILAS
Firstly, UKDILAS provides thorough lactation-specific information on individual medications. When a health professional wants to check a single medication, where they would normally look it up in the BNF, they can go to www.sps.nhs.uk (or Google UKDILAS) and use the search box at the top of the page:
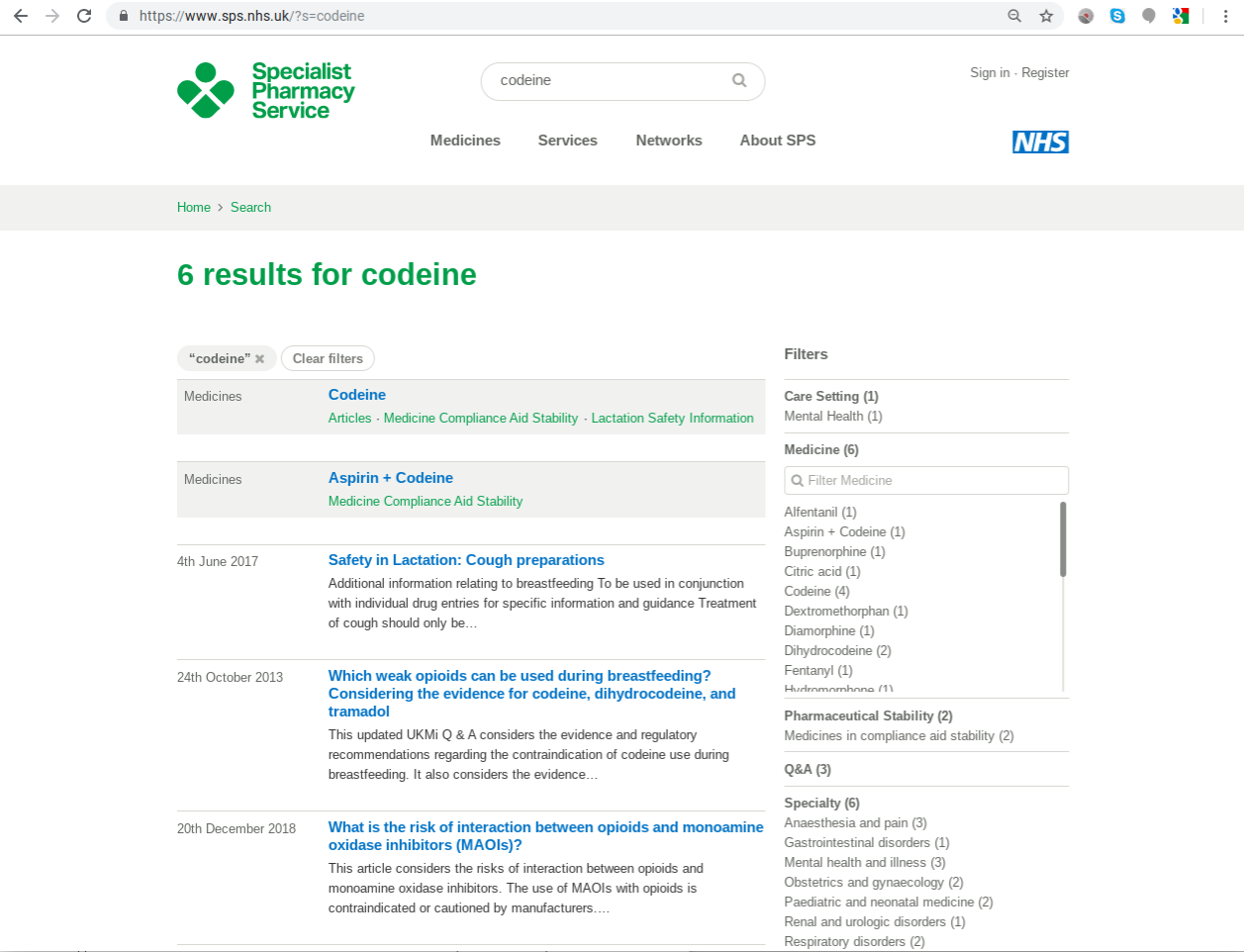
Searching for codeine, for example, will bring up first the individual drug name and any lactation (and other specialist service) factsheets as well:
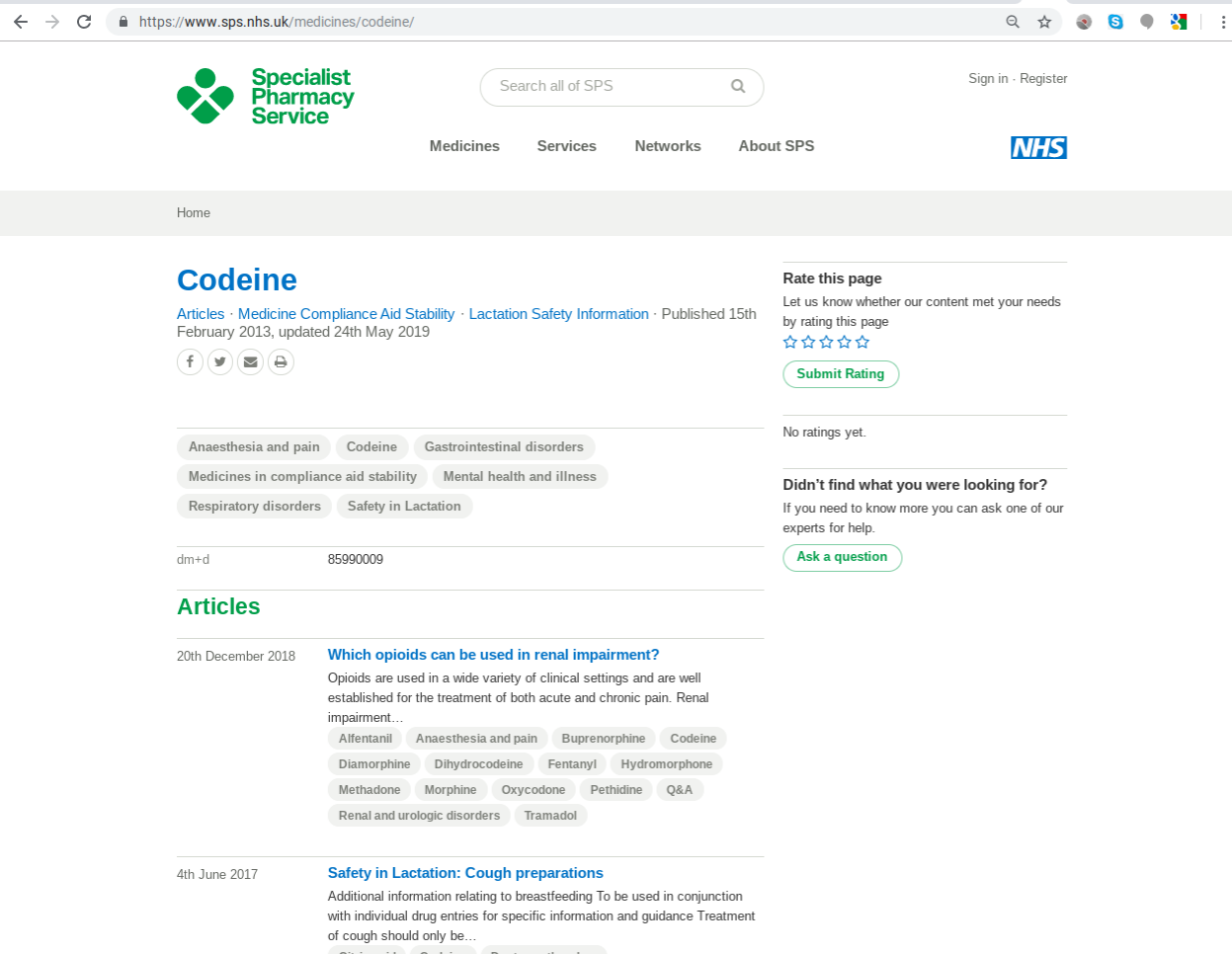
Clicking on the individual drug name codeine brings the reader to a long list of articles and other specialist information so the last step is to click on the “Lactation Safety Information” link under the medication name to go straight to the relevant section.
In this case, the final result is “Use when breastfeeding – No” with useful comments about how much data this is based on and what effects are seen. This will also link you through to any other relevant lactation safety information held about this medicine:
The other two UKDILAS services are the factsheets and the ability to ask specific questions. Question & Answer factsheets are available via a link from the UKDILAS part of the SPS website (www.sps.nhs.uk/ukdilas) and cover general topics like “which oral antihistamines are safe to use while breastfeeding?”. There are also general “safety in lactation” articles covering specific classes of medication – these will come up when you search for an individual medication, as shown above with codeine, which is an opioid analgesic.
To ask UKDILAS a specific question, health professionals can telephone (9am-5pm Mon to Fri) or email – full details are on the website. The team will answer any breastfeeding and medicine-related question, but particularly specialise in highly complex areas such as multiple medications and premature infants.
Other sources of information on drugs in breastmilk
As lactation professionals know, there are many other ways to access information about medications in lactation – for example the wonderful Drug Factsheets put together by Wendy Jones at the Breastfeeding Network, American national resource LactMed and textbooks such as Medications and Mothers’ Milk (Hale). This blog has focused on UKDILAS because it is an NHS source, which is reassuring to busy UK health professionals who may not have time to check the credentials of other sources.
So, in summary, health professionals naturally use the BNF to check information about lactation, but by using the Don’t Say Stop Look It Up campaign, we can help them find out about specialist sources of information to help families make informed decisions.
Ilana Levene is a paediatric doctor planning to sub-specialise in neonatal medicine and interested in research relating to neonatal nutrition. She lives in Oxford with her husband, an environmental consultant, and two children. She is a trustee of Oxfordshire Breastfeeding Support, a local grassroots network of free weekly breastfeeding drop-ins and online support. She likes cross-stitching and making patchwork quilts.