WBTi UK Steering Group members, Helen, Clare, Alison and Patricia, were very pleased to be invited to give a presentation on the 2024 Report to the All-Party Parliamentary Group (APPG) on Infant Feeding on 18 June, 2025. This APPG, an informal cross-party group, is hosted by Liberal Democrat MP for Chichester, Jess Brown-Fuller, who is a staunch advocate for breastfeeding. Meetings are quarterly.
(left to right) Jess Brown-Fuller MP, Helen and Patricia during the presentation
The hybrid event was held in Portcullis House, which is close to the Houses of Parliament and overlooks the River Thames.
At the meeting, Helen and Patricia gave an overview of the Report’s findings. This triggered a range of questions from the audience in the room and online. Attendees included Labour MP for Ribble Valley, Maya Ellis, and Liberal Democrat MP for mid-Sussex, Alison Bennett, along with representatives of Royal Colleges and local public health teams, as well as the breastfeeding support organisations.
(left to right) Jayne Joyce and Emily Lunny (LLLGB), Helen Gray and Patricia Wise (WBTi Steering Group) and Katie Pereira-Kotze (First Steps Nutrition Trust)
Presentation title slide
APPG meetings
If you would like to be notified about future Infant Feeding APPG meetings, please contact Edmund Legrave, Parliamentary Assistant for Jess Fuller-Brown: edmund.legrave@parliament.uk
August 1-7th marks the World Breastfeeding Week. The theme is ‘Let’s make breastfeeding and work, work!’ The benefit of breastfeeding to health, the economy, work and the environment is widely documented. However, the UK remains one of the countries in the world with the lowest breastfeeding rate. Although 81% of mothers set out to breastfeed, only 1% of babies in the UK are still exclusively breastfed at 6 months. The question has always been why is breastfeeding rate so low in the UK?
Photo credit: Dr Paige E. Davis
Return to work is one of the key barriers to breastfeeding especially where the workplace is not breastfeeding friendly. A study published in 2007 by the Cohort Group found that mothers employed part-time or self-employed were more likely to breast-feed for at least 4 months than those employed full-time. The longer a mother delayed her return to work postpartum, the more likely she was to breast-feed for at least 4 months. Mothers were more likely to breastfeed for at least 4 months if their employer offered family-friendly or flexible work arrangements, or they received Statutory Maternity Pay plus additional pay during their maternity leave rather than Statutory Maternity Pay alone. This demonstrated that return to work could have a negative impact on breastfeeding if the mother is not properly supported.
Currently the UK does not have a legal framework that protects and promote breastfeeding in the workplace. The 1001 critical days strategy is there but does not have a legal backing to ensure that mothers are properly supported to continue breastfeeding should they choose to return to work early. A general assumption is made that mothers would take the full 52 weeks of maternity leave even though the leave is not properly paid. Mothers returning to work find it challenging to understand what they can and cannot do.
Though many employers are quick to showcase how family friendly they are in supporting working parents, breastfeeding remains an area in need of significant improvement. This is predominantly because the government has failed to recognise the benefits of breastfeeding and has failed to embed it in the current family friendly rights. Ideally, maternity leave should naturally go with a workplace breastfeeding policy. Other family friendly policies such as shared parental leave is not achieving its desired impact partly because of the lack of breastfeeding support in the workplace.
Mothers who intend to breastfeed for long may not share their maternity leave with their partners if support is not in place in the workplace.
Our other WBTi blogs on maternity protection and breastfeeding breaks in the workplace HERE and HERE
Mandate all large public places like shopping malls, community centres, public libraries, museums, etc to provide breastfeeding rooms or spaces.
Fully adopt The Code of Marketing of Breastmilk Substitutes to protect babies and their families from harmful commercial influences and undermining of breastfeeding for commercial profit; and to protect families who formula feed from the escalating costs of premium brands.
Our WBTi 2016 findings and recommendations on Indicator 3: The International Code that the UK government implement the full Code and subsequent relevant WHA Resolutions in UK law and regulations, and also monitor and enforce these regulations.
Provide adequate 24/7 specialist lactation support in maternity services to actively counteract the culture of formula top-ups in hospitals; and to enable human donor milk to be more accessible as an option when mother’s milk is not immediately available.
Guarantee a sustained funding support to breastfeeding organisations who play a key part in supporting mothers.
Include breastfeeding support on the Net Zero Environmental Agenda.
Dr Ernestine Gheyoh Ndzi is the Associate Dean for Law and Police Studies at York St John University. Her research interest lies in Company Law and Employment Law. Ernestine has in the past four years been researching on shared parental leave and breastfeeding. Ernestine is a member of the Board of Trustees for The Breastfeeding Network. She is the producer of the breastfeeding documentary titled ‘Breastfeeding: Not on the Agenda. She is running a 9-webinar series exploring the benefits and challenges of breastfeeding. She is also leading on the campaign for change to support breastfeeding in the UK.
When you think of the UK Armed Forces, many of our minds will go to an infantry soldier fighting stoically on the battlefield, or perhaps bearskins guarding the King at the palace. Not many people think of breastfeeding mother. But we do have them.
The Defence Breastfeeding Network launched in June 2020, to support breastfeeding soldiers during their maternity and return to work phase. Initially, we started with a Facebook group for some community support. We then created a partnership with Families and Babies Lancashire, who train members of the DBN to become level 2 breastfeeding peer supporters. As a network, we have currently trained over 60 peer supporters who give back to our members but also in their own communities. A project the DBN is currently working on is the establishment of breastfeeding/ wellness rooms within our infrastructure. These rooms all have a lockable door, comfortable seating, access to fridge space, access to clean running water and electricity. Many of the rooms are made comfortable with extra facilities such as tea and coffee stations, TV’s/radios, microwaves and more, with credit to the individuals within units that set these rooms up for all to benefit from. These rooms are more than just set up for those that need it now, they’re set up for when they are needed in the future. As an organisation, the Armed Forces are setting an example that I would encourage every employer to follow.
In 2021, the Defence Breastfeeding Policy was launched, providing clear and concise information for line managers on how to effectively manage and support breastfeeding mothers in the workplace, from risk assessments to medical gradings and through to deploying into a field environment which can mean living outside for extended periods of time. This does not mean we are sending breastfeeding mothers away from their children for months on end with little notice but takes into account the fact that we are soldiers, aviators and sailors. Gone are the days where women were dismissed from the military for being pregnant, and now as an organisation we are aiming to be proactive with breastfeeding support rather than reactive. Service life isn’t always easy on the service person or their immediate family, and as a network, the DBN is there to be as much of a village as possible. Education is really important, and the DBN attends unit health events and gives briefings across the UK to raise awareness of policy and the networks existence, in order to create more allies within the Armed Forces.
I have personally been on a field exercise (in the UK) with a manual breastpump in my bergen. It was handled wonderfully, I was able to take a small fridge to store my milk and was able to be transport it back to a freezer too. I was given the time, space and respect to express milk comfortably and was treated with dignity. I went on to feed my son for 2.5 years.
So how do we make breastfeeding work? We need support. We need employers that are proactive and view mothers as an asset and not a hindrance. We need support from everyone else; our families, friends, and strangers in the street. And I’m proud to say that the Armed Forces is a great champion.
LCpl Natasha Day MBE joined the British Army in 2014 as a Combat Medical Technician, deploying to South Sudan and Kenya before studying to become a Paramedic in 2021. After the birth of her son Charlie, she established the Defence Breastfeeding Network (DBN) in 2020 to support members of the Armed Forces and their families in their breastfeeding journey. The DBN supports over 1300 families and has collectively opened 83 breastfeeding and wellness rooms across Defence infrastructure. Natasha is currently posted to the NHS as a Paramedic.
Imagine if every mother was entitled to the paid maternity leave, breastfeeding breaks and flexible return to work options she needed to enable her to combine breastfeeding with earning an income.
Please join the Global Breastfeeding Collective at a webinar to celebrate World Breastfeeding Week. Maternity leave and workplace accommodations are critical features of environments that enable breastfeeding. Hear from mothers about their experiences combining work and breastfeeding, get new ideas from countries who have used evidence-based policies to make breastfeeding work, learn about updated maternity leave recommendations, and find resources to support advocacy.
The Global Breastfeeding Collective is a partnership of more than 20 prominent international agencies, including the World Health Organization and UNICEF, calling on donors, policymakers, philanthropists and civil society to increase investment in breastfeeding worldwide.
August 1-7 will once again be World Breastfeeding Week. This year, the theme “Enabling Breastfeeding: Making a Difference for Working Parents” is all about combining working and breastfeeding.
One of the key findings from our first WBTi assessment of UK breastfeeding policies and programmes was that although the UK does provide paid maternity leave, and some paid paternity leave, and although there is some guidance on good practice from ACAS and from HSE, there is no statutory right in the UK to breastfeeding breaks or facilities in the workplace.
WABA produces regular snapshot Parents at Work reports on each country’s status on implementing International Labor Organization (ILO) conventions and recommendations on maternity protection at work, including maternity leave, paternity leave, and protected breaks for breastfeeding or expressing milk.
Breastfeeding-friendly workplaces provide time, income security and space to enable positive nutrition and health outcomes
All women should have the right to paid working time for breastfeeding, as called for by ILO Convention No. 183. In 2021, 138 countries provide a right to time and income security for breastfeeding. These provisions potentially benefit 8 in 10 potential mothers across the world. Since 2011, seven countries have introduced paid nursing breaks. However, breastfeeding breaks remain unpaid in four high-income countries. In 2021, at least four pathfinder countries recognize men’s supporting role by offering breastfeeding breaks to fathers.
Almost 5 in 10 potential mothers live in countries that grant two daily breastfeeding breaks; while 109 countries offer the right to daily nursing breaks for six months or more. This would support exclusive breastfeeding in line with World Health Organization (WHO) recommendations for 7 in 10 potential mothers across the world. However, only ten countries provide a right to breastfeeding breaks for at least two years, compromising mothers’ ability to continuing breastfeeding.
Workplace nursing facilities are a key ingredient of breastfeeding-friendly workplaces. However, only 42 countries offer the right to workplace nursing facilities, covering roughly 6 in 10 potential mothers globally. While small- and medium-sized enterprises (SMEs) are often exempted from these requirements, research shows that the economic and well-being benefits of breastfeeding for the new-born, the mother and the employer outweigh the limited costs of these measures. Only 13 countries offer a right to workplace nursing facilities irrespective of the number and sex of workers, with only 5 in 100 potential mothers worldwide living in these countries. Conditionalities for nursing facilities based on sex are discriminatory and remain in place in 19 countries.
WBW Action Folder
Details for campaigning for improved policies and support for breastfeeding in the workplace can be found in the World Breastfeeding Week Action Folder.
WBW Pledge Map
Organising a WBW2023 celebration? Add it to the pledge map!
Previous webinars in the series and the documentary are available on YouTube.
Thursday 3rd August at 1pm
‘Let’s make breastfeeding work – optimal maternity leave and workplace accommodations support an environment that enables breastfeeding’. Free webinar from the Global Breastfeeding Collective, led by WHO and UNICEF.
Maternity Action’s Senior Policy Officer Annah Psarros, on their new Toolkit for Employers, including a model Breastfeeding Policy
Saturday 5th August
Dr Ernestine Ndzi on Shared Parental Leave
Sunday 6th August
LCpl Natasha Day MBE, founder of the Defense Breastfeeding Network
Monday 7th August
Final blog from Dr Ernestine Ndzi on the need for “Family-Friendly Policies at Work”, and a Call to Action
Petition
And finally, everyone is encouraged to sign and share this petition from Dr. Ernestine Ndizi, calling for the government to:
Embed breastfeeding in the school curriculum and relevant health professional training.
Provide a policy on breastfeeding in the workplace which will protect the rights of breastfeeding mothers in the workplace.
Mandate all large public places like shopping malls, community centres, public libraries, museums, etc to provide breastfeeding rooms or spaces.
Fully adopt The Code of Marketing of Breastmilk Substitutes to protect babies and their families from harmful commercial influences and undermining of breastfeeding for commercial profit; and to protect families who formula feed from the escalating costs of premium brands.
Provide adequate 24/7 specialist lactation support in maternity services to actively counteract the culture of formula top-ups in hospitals; and to enable human donor milk to be more accessible as an option when mother’s milk is not immediately available.
Guarantee a sustained funding support to breastfeeding organisations who play a key part in supporting mothers.
– Include breastfeeding support on the Net Zero Environmental Agenda.
A network of trained peer support is an essential part of high quality integrated breastfeeding services.
Unicef UK Baby Friendly Initiative (BFI) outlines three components that good local breastfeeding services must include, in order to be awarded Baby Friendly accredited status.
Basic, or Routine Care
All health workers who work with new families (health visitors and any allied healthcare assistants in the community services) have been trained to BFI standard (approximately 18 hours of initial in service training, with yearly updates of an hour or more).
Additional services
Here BFI outlines how every health visiting and community service must be embedded in and well supported by a network of trained peer supporters, or other social and trained breastfeeding support. NICE recommends that peer support programmes be externally accredited. Good practice includes not only training, but also regular supervision and updates of skills and knowledge. Typical peer support programmes require peer supporters to be experienced breastfeeding mothers, and often expects them to come from similar communities as the population they are supporting. Training generally is part time, over 16-36 hours. Peer supporters work in a supervised setting, acting as an “informed friend,” and referring complex cases on to health professionals or an advanced breastfeeding practitioner such as an IBCLC or breastfeeding counsellor, using a referral pathway.
Breastfeeding counsellors in the UK are also experienced breastfeeding mothers, so they also provide a type of peer support, or “mother-to-mother” support. Their training typically take around two years, and they are autonomous practitioners, who can be responsible for leading their own local breastfeeding support groups, usually through one of the main UK breastfeeding voluntary organisations.
Mothers who are experiencing breastfeeding challenges often need more than one visit – and they need the time that it requires for skilled listening as well as exploration of possible breastfeeding strategies to resolve the issue. Although many health visitors have additional breastfeeding training and skills, the health visitor workforce is vastly overstretched, and it simply isn’t possible to provide the time and the number of visits that many breastfeeding mothers need.
But peer support programmes can provide this – they offer groups where lonely mothers can meet others and gain confidence in their own mothering, alongside skilled listening and well- informed support. Many mothers will find their own “village” in their local breastfeeding support group, and will return again and again. Some will go on to train as peer supporters or breastfeeding counsellors themselves.
Peer support groups are the beating heart of breastfeeding support
Helen Gray, WBTi Joint Coordinator
WBTi audit of peer support and breastfeeding counsellors provided by the voluntary sector, 2016 In Part 2 of our WBTi UK Report
Specialist support
Every area should have a referral pathway to specialist care at the IBCLC (International Board Certified Lactation Consultant) or similar level, for those complex cases where breastfeeding issues cannot be resolved at the level of basic/ routine care or by additional peer support.
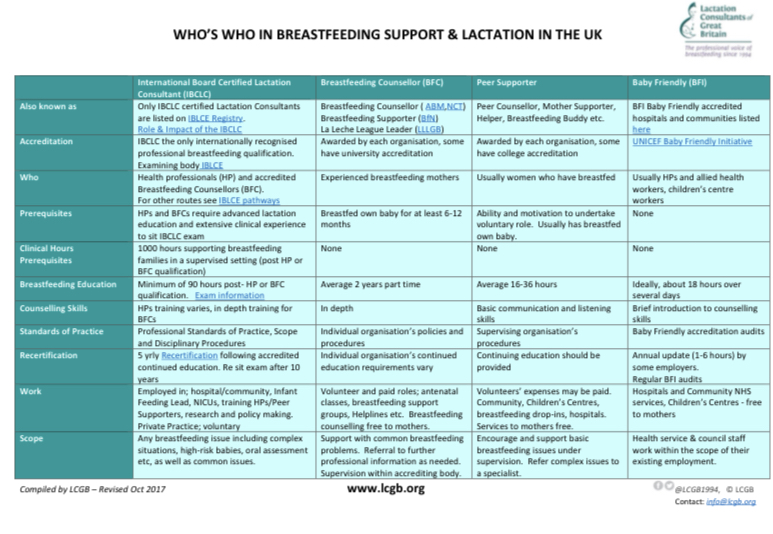
The different roles of breastfeeding support in the UK have been outlined in the chart below:
WBTi’s research: Case studies of best practice The WBTi 2016 Report featured several case studies of areas who showed best practice in providing well joined up, integrated breastfeeding services: Brighton and Harrow.
More recently, our WBTi team has presented posters featuring these and additional case studies of best practices in providing integrated breastfeeding services: Medway, Harrow and Swindon.
WBTi Poster on Integrated Breastfeeding Services.
These examples of best practice in integrated breastfeeding services gave concrete results.
They demonstrated:
– a 2% rise in breastfeeding rates in a socially deprived area in 2018 (Medway),
– a 15% rise in initiation and a 12% rise in continuation of breastfeeding over a six year period (Harrow)
– and a 6% reduction in drop off rates from birth to 6-8 weeks over six years (Swindon).
Our WBTi team are always on the lookout for further examples of best practice in integrated breastfeeding services, and we submit them to Public Health England. Please do contact us if you would like to submit your local services!
Helen Gray MPhil IBCLC is Joint Coordinator of the World Breastfeeding Trends (WBTi) UK Working Group. She is also an accredited Leader (breastfeeding counsellor) with La Leche League of Great Britain.
Guidance is needed on infant and young child feeding for families in the UK affected by disasters and emergencies.
Heather Trickey and Helen Gray.
Disaster and emergency situations – floods, fires, terrorist attacks and widespread power failures – can affect any country, including the UK. In any disaster or emergency, babies are vulnerable and continued access to adequate and safe nutrition is essential. Families need support to ensure that children continue to be cared for and fed in line with their needs.
There is no UK government plan
The World Health Assembly (WHA Resolution 63.23) has recommended that all countries implement existing global guidelines on infant feeding during emergencies, including specific operational guidance to help relief agencies protect infant nutrition and minimise risk of infection. Although there is national guidance on care of animals during emergencies, a recent World Breastfeeding Trends Initiative (WBTi) report found that there are no UK-wide or national strategies addressing infant and young child feeding during a disaster. Scotland is the only part of the UK that has a named lead on infant feeding in emergencies. Emergency planning and response is devolved to local authorities; because there is no guidance on the protection of families with infants there is no way to ensure that local strategies consider infant nutrition as part of emergency response.
Risks for formula fed babies
Babies who are fully or partially formula fed are at risk if their caregivers lose access to clean water, are unable to sterilise feeding equipment or suffer disruption or contamination of their formula milk supplies. A suitable environment for preparation and storage of feeds, sterilising equipment, boiling water and safe storage such as a refrigerator, are all needed to prevent bacterial contamination
Emergency supplies required to care for and feed a formula fed baby for one week in a developed country, using read-to-feed milk. From Gribble & Berry 2011 “Emergency Preparedness for those who care for infants in developed country contexts.” International Breastfeeding Journal /2011 6:16
Risks for breastfed babies
Breastfeeding protects against infection and can be comforting to infants and mothers during difficult times. Mothers’ supply of breastmilk is resilient, however, chaos, displacement and emotional strain, coupled with commonly held misconceptions about how breastfeeding works, can undermine a mother’s confidence and result in less frequent feeding. Breastfeeding mothers need access to the option of feeding in a private space and reassurance that continuing to breastfeed is the best option for their baby.
Skilled support can help mothers resolve breastfeeding problems and maintain the protective effect of full or partial breastfeeding. If breastfeeding helpers are not pre-authorised as part of planned disaster response the immediate help that families need can be delayed.
Risks associated with donated formula milk
The world is a better place than we sometimes think. When a disaster strikes, ordinary people often respond with an outpouring of generosity. We give clothes, equipment and food spontaneously and in response to public calls.
Donations of clothing, bedding, toys, food and water, London, June 2017. Photo Credit: @balhammosque
In the absence of guidance, agencies responsible for co-ordinating emergency response and volunteers working on the front line are often not aware that donations of formula milk can put babies at risk. Risks from donated formula milk include inadvertently distributing products that are unsuitable for babies under six months or for babies with special nutritional needs, as well as distributing milk that is contaminated or out-of-date. There is also a risk that donations will be inappropriately provided to parents of breastfed babies, which can undermine the protective effect of breastfeeding and cause parents to become dependent on a continued supply of formula milk.
International guidelines for emergency feeding caution against accepting donations of formula milk. It is recommended that emergency planners and first responders, with expert advice, take responsibility for purchase and distribution of appropriate formula milks in line with the needs of each family.
What’s been done so far?
International guidelines for protecting infants in disasters and emergencies are available. There is a need to adapt these to a UK context, where, beyond the early weeks, many babies are fully or partially formula fed and which includes a rich mix of cultures and nationalities with different feeding practices.
UK-based emergencies have tended to be highly localised and short-term. However, UK guidance will need to ensure preparedness for longer-term support needs, for UK charities and for displaced families and unaccompanied children who have sought refuge from outside of the UK.
Several UK agencies have developed guidance with limited scope. The Food Safety Agency has issued guidance to support safe preparation of formula milk in response to flooding and contamination of local water supplies. [20222 update: UNICEF UK Baby Friendly Initiative has produced guidance for Local Authorities on supporting families with infants who are experiencing food insecurity]
[2021 update: See also the infographic series from the Infant Feeding in Emergencies Core Group on managing appropriate infant feeding interventions during emergencies, including Preventing and managing inappropriate donations during emergencies: https://www.ennonline.net/ifecoregroupinfographicseries]
How to help ensure babies’ nutritional needs are protected
In the absence of national guidance, relief co-ordinators and agencies and members of the public will be concerned to do the right thing in response to a disaster. There is an urgent need to improve planning and raise awareness about the best ways to support infant and child feeding. These key points from have been adapted from UK and international guidance:
1) Members of the public
DO donate money to key agencies. This is the best way to support parents who need to buy formula milk. Money will allow parents, caregivers or coordinating aid organisations to buy the most appropriate milk to meet the individual needs of each baby. Donated formula milk can inadvertently put babies at risk.
DO offer your time to help agencies co-ordinating relief. Support and encourage mothers who are breastfeeding. Breastfeeding is protective against infection, and provides the baby with the safest possible nutrition.
2) Relief workers and aid agencies
DO have a local plan to support infant and young child feeding in emergencies in place for local authorities, first responders and aid agencies. All families should be screened to ensure they receive appropriate support or supplies.
DO ensure that mothers who are fully or partially breastfeeding have the support they need to continue. Mothers can seek support from their midwife or health visitor. Local emergency planning should have identified appropriate infant feeding support from local health and voluntary services. There are telephone helplines which support caregivers with all aspects of infant feeding:
NCT helpline (0300 330 0700)
The National Breastfeeding Helpline (0300 100 0212).
DO encourage donations of money to recognised agencies so that parents, caregivers and agencies can buy any formula or supplies needed, rather than donations of formula products.
Appropriate support or supplies including cash cards specifically for the purchase of infant formula and complementary foods for young children could be considered.
DO ensure that formula milk is purchased and distributed only for babies who need formula milk, following basic screening of families (simple triage tools have been recently been developed for use in emergency situations in Greece and Canada).
DO NOT distribute formula milk in an untargeted way.
DO ensure that parents are aware of guidance on sterilisation of bottles and teats and how to prepare any powdered formula safelyand have access to facilities to carry this out, to reduce the risk of contamination. Liquid ready-to-feed formula may be needed if suitable preparation facilities are not available.
What is needed now?
There is an urgent need for UK governments to ensure infant and child nutrition is protected as part of the planned new strategy for resilience in major disasters. Local authorities and relief agencies require national guidance to develop local strategies so that we can all be better prepared.
Heather Trickey is a Research Associate based in DECIPHer, Cardiff University. Her research focuses on public health policy and parents, particularly Infant Feeding Policy.
Helen Gray is Joint Coordinator of the World Breastfeeding Trends (WBTi) UK Working Group.
Support is the theme for National Breastfeeding Celebration Week in England this year. Mothers are sharing their photos and stories of key support from their own “breastfeeding best friend” on social media with the hashtag #bffriend17
Who was YOUR “breastfeeding best friend”? #BFfriend17?
Ruth’s experience is typical: “[Day 6 after the birth, 4am] Me – sobbing: I don’t think this latch is right. It hurts. No, it really hurts. It’s not supposed to hurt. I’m sure it’s not supposed to hurt. But he’s hungry. I have to feed him. I need help. I’m tired, and I’ve got no idea what I’m doing. Who can I get help from?
First time breastfeeding mums the country over will recognise this. The pain of a poor latch, a hungry baby, knowing you need help and not knowing where to get it. At 4 AM, in a state of nearly delirious sleep deprivation. I hung on until the morning, when my dad brought my ex-midwife grandma to help me. She showed me how to relieve my engorgement and soften my nipples so that my baby had something to latch on to. Though it wasn’t totally plain sailing from there. The several days of poor latching had given me a badly cracked nipple, and then I got mastitis. But it healed, and I went on to breastfeed for 2 years. If I hadn’t had my grandma’s support at that moment, I would have stopped breastfeeding.”
So how exactly do we – in England – support breastfeeding mums? There is support available. They can access support from midwives, health visitors, lactation consultants, breastfeeding counsellors and peer supporters. This might be through the NHS, or via third sector organisations such as the Association of Breastfeeding Mothers, the Breastfeeding Network, La Leche League and NCT. (Indicator 6 in the WBTi report, Part 1 and Part 2) There have, however, been significant cuts to many of these services, particularly peer support and drop-ins (part 2, page 30) and there was already a huge postcode lottery in the services available. This is compounded by the fact that there is no national information and communication strategy in England (Indicator 7). There is no centralised database of breastfeeding drop in support (the NHS Choices “find local support” (http://www.nhs.uk/service-search/Breastfeeding-support-services/LocationSearch/360) service uses information held by Netmums) So while there is support available, it can be difficult to find and difficult to access, and in many areas there is just not enough. And it’s certainly very difficult at 4 AM in the middle of a feeding crisis.
Commissioners to ensure there is a range of integrated postnatal services that include both health professional and voluntary-sector breastfeeding support, meet local needs and provide clear access to specialist support.
Government to implement existing NICE guidelines on antenatal and postnatal breastfeeding information and support.
Government to make Baby Friendly accreditation in all maternity and community settings mandatory.
Commissioners to maintain the full range of health-visiting services, and maintain health visiting as a universal service.
Funding for public health to be protected.
PHE to explore options to enable families to access information about local services.
Governments to improve data collection to aid evaluation of services.
Government needs to create a national communications strategy to:
provide accurate information in publications and online sources, liaising more with relevant organisations;
include WBW/National Breastfeeding Celebration Week;
launch a public information campaign aimed at wider society (family, community, workplaces).
DH to update the NHS Choices website to provide accurate information and details of breastfeeding support organisations.
A joined up service which meets the individual needs of each mother is essential to properly support mothers to breastfeed. Different mothers need different levels of support and their needs vary during their breastfeeding journeys. On some occasions an understanding friend is enough, sometimes a peer supporter and on others a highly skilled lactation specialist is needed. When we fail to meet these needs, we fail families. It is time for this to stop. It is time to properly support women in their choice to breastfeed their babies. Who was YOUR #bffriend17?
Post your own selfie with YOUR #bffriend17 on Twitter, Instagram, or facebook!
A #BFfriend can change your life!
Dr Ruth Stirton is a Lecturer in Healthcare Law at the University of Sussex. She works on healthcare regulation, She is an admin of the My breastfeeding Story facebook group and is currently breastfeeding her second child.
If you attended the 2015 Unicef UK Baby Friendly conference you may have noticed, or taken part, in the informal World Breastfeeding Trends Initiative (WBTi) competition to guess the final assessment score. Sue Ashfield is the winner as her estimate was closest to the actual score of 50.5 out of 100 for Indicators 1-10.
The score is a measure of how the UK is performing against the implementation of key policies and programmes to support mothers who want to breastfeed and the healthcare professionals who help them.
Sue is the lead and Specialist Health Visitor (Infant Nutrition) of First Community Health and Care in East Surrey. Sue is a winner in a much bigger way than the WBTi competition because her community team was reaccredited by Baby Friendly earlier this year and they also supported 10 local children centres in achieving full BFI accreditation in one year. The formal presentation of the award was on March 14th. Sue pays tribute to the hard work of her colleagues for the achievement but it also reflects her commitment and leadership. Read more here.
Her team is a brilliant example of what the WBTi UK report recommends for Indicator 6 (community-based support). There is close, integrated working between 0-19 public health team, breastfeeding counsellors, peer supporters and children centres at the three Baby Cafes, which have been runnning for 10 years.
Practitioners from the 0-19 team work at the Baby Cafes on a rota basis, alongside the breastfeeding counsellor. When they see mothers at home or at drop-in clinics they encourage them to attend the Baby Cafes for social support or more specialised support or just to chat to one of the peer supporters. The breastfeeding counsellors at the Baby Cafes have now trained over 200 peer supporters and this has increased the breastfeeding knowledge and skills within the local community.
Credit: Eleanor Stock
The photo above shows Sue holding the Baby Friendly Initiative (BFI) accreditation plaque along with some members of the 0-19 team, some senior managers and their BFI Guardian. Since April, all three community services in Surrey have come together as Children and Family Health Surrey to deliver children’s services.
Sue comments that she found particularly useful the information in the WBTi report about interventions and investment offered in the past and also Report Cards and the summary gaps and recommendations. She will use the findings in the report to inform local commissioners and disseminate information to staff and other stakeholders.
An integrated service like this is needed in all areas, yet in so many places services are being cut, particularly peer support programmes and breastfeeding support drop-ins.
Many congratulations Sue.
Cover photo credit: Paul Carter
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group
The inspiring story of breastfeeding support in a London borough
What changed?
I have been reflecting recently on my experiences as a specialist health visitor and infant feeding lead in an outer London borough. The story began twelve years ago, in 2005, when there was a lack of confidence among mothers and staff about the reliability of breastfeeding, which was hidden and rarely seen in public. Over the next eight years, the initiation rate increased from 67% in 2005 to 86% in 2013, and the continuation rate at 6-8 weeks from 50% to 75% (52% breastfeeding exclusively). Breastfeeding became the way most mothers fed their babies. Gradually breastfeeding mothers became visible in cafes, shopping centres, supermarkets, streets, GP surgeries and children’s centres. The Unicef Baby Friendly Initiative assessors stated in a report that, in this borough, breastfeeding had become ‘the normal way to feed babies’.
How did it happen?
How did this change come about in a relatively short period of time? It began in 2005, as a joint project between the NHS and NCT, which secured local health authority funding to set up a breastfeeding support group in an area of social deprivation with low breastfeeding rates. This group became very well attended and was facilitated effectively by two NCT breastfeeding counsellors and a health visitor. A similar group was set up in another part of the borough and was run by me, together with other health visitor colleagues. Many of the mothers were very grateful for the support they received in the groups and some of these women expressed the wish to train as volunteer peer supporters, so that they could help other mothers enjoy breastfeeding their babies, as they had. Two training courses were organised and, that year, 20 peer supporters were trained, registered by the voluntary services of the local Primary Care Trust (PCT), and started working in breastfeeding support groups, in the children’s centres and health service clinics. The news of the training spread rapidly and soon there was a waiting list of mothers wishing to train!
Reaching out
The numbers of groups expanded to be easily accessible to mothers across the borough, running every weekday, in children’s centres, cafes, and health premises. The new peer supporters brought fantastic skills with them, one setting up a website, another a mothers’ Facebook page and another designing our leaflets and posters! One had breastfed twins and set up antenatal sessions for parents expecting multiple births plus a weekly support group for mothers with twins and more. She also visited these mothers at home and lent them cushions, which helped them tandem feed. Soon the exclusive breastfeeding of twins and even triplets became common. A group of Somali mothers was trained and an outreach peer supporter started seeing Somali pregnant women in the hospital. A teenage ‘buddy’ scheme was also started by some of the younger peer supporters, working with the specialist midwife and running antenatal sessions and postnatal support for young mothers. Two peer support co-ordinators were employed to job-share this important role and to deal with concerns of the peer supporters as well as helping with training and supervision. Over the next ten years, more than 200 voluntary peer supporters were trained in the borough and the training continues until the present day.
Unicef UK/Mead
Public Health prioritises breastfeeding
In 2006, under the government scheme of “Every Child Matters’, the Director of Public Health made breastfeeding the top priority for all children in the borough with accompanying ‘stretch targets’ and funding.
London services are monitored through the ‘Good Food for London’ report on their Baby Friendly status, with details on how each borough is achieving and sustaining the Baby Friendly standards
Baby Friendly accreditation
In 2012 Unicef UK Baby Friendly Initiative carried out a major review that resulted in new, more holistic, child rights-based standards relating to the care of babies, their mothers and families, with a strong emphasis on building responsive loving relationships. A new award has also been introduced to encourage a focus on sustainability after the accreditation.
In parallel with the rapidly increasing numbers of peer supporters, the journey in the borough to become Unicef Baby Friendly (BFI) accredited started and professional training in the community and local hospital began with the two health trusts starting their journeys jointly. A model of multidisciplinary training of midwives, maternity assistants, neonatal nurses, nursery nurses and health visitors began initially with BFI-facilitated training. This enabled hospital and community staff not only to improve their breastfeeding knowledge and skills, but also each other’s roles, co-operate on work challenges and break down any barriers which may have existed previously. Communication skills and talking about their own life experiences, in order to gain an understanding of their impact, especially with infant feeding, became an important part of the in-service training. Interactive group exercises on different breastfeeding situations became an integral part of the training, emphasising the importance of empathy and seeing the problems through the eyes of the mothers. A neonatal breastfeeding co-ordinator was appointed and started training all the neonatal staff in the hospital, including the doctors, and by 2014, Unicef had awarded both the community and hospital trusts their Baby Friendly accreditation.
Peer support
Peer supporters were also employed by an adjacent borough to work in the hospital, supporting mothers on the postnatal ward, one even working all night once a week; others taught hand expressing and colostrum harvesting in the antenatal clinic, especially for mothers with diabetes.
Unicef UK/Mead
Achieving cultural change
Within ten years, breastfeeding became a normal and accepted way to feed babies in the borough. Mothers, fathers, and grandmothers-to-be came in large numbers to the twice monthly breastfeeding workshops, gaining confidence and information, with the expectation of the support that would be available to them to help them achieve their goals. A mother said ‘the session expelled myths and I now know how milk is made and transferred to my baby. I am looking forward to skin-to-skin contact after the birth and will follow my baby’s instincts’. Parents meet peer supporters in the support groups, at toddler groups, in the school grounds, in cafes, at sports events, in churches, temples, synagogues and mosques. Peer supporters live and work in the community and spread their knowledge through everyone they meet. Even when they move away from peer support, they take their embodied knowledge into the work place and support their colleagues there. Cultural change can happen through peer support, resulting in breastfeeding becoming embedded in a community. This change is sustainable over time and in future generations, as it spreads through different social groups. Voluntary peer support and informed, professional support is capable of changing attitudes and behaviour within a community to make breastfeeding ‘normal’ in a very cost-effective way. Commissioners need to be aware of how health outcomes can be improved through breastfeeding, for mothers and children, in the immediate and long-term, and it is essential to protect and increase future funding for midwives, health visitors and peer supporters, in order that vital programmes like this can continue.
The World Breastfeeding Trends Initiative UK report in 2016 affirmed the borough’s actions as it recommends in Indicator 6 (Community-based support) that ‘commissioners ensure that there is a range of postnatal services that include both health professional and voluntary-sector breastfeeding support to meet local needs and provide clear access to specialist support’ and that they ‘maintain the full range of health visiting services, and maintain health visiting as a universal service’. Indeed, the borough’s transformation in breastfeeding support is used as a case study in Part 2 of the report.
One mother with an eight-month old baby told me:
‘I so much wanted to breastfeed, but found it incredibly hard at the beginning. I was convinced that it wouldn’t work and it was such a lonely feeling, like I was failing where other mothers were succeeding. Getting support made all the difference- having someone to listen to me and give me confidence to carry on. Suddenly, I didn’t feel alone any more and it changed everything. I know that I would not be breastfeeding now if I hadn’t got help in those crucial first weeks.’
What one London borough has achieved shows what is possible. Unicef UK Baby Friendly Initiative’s Call to Action spells out four key actions to create a supportive, enabling environment for women who want to breastfeed, ranging from national strategy and legal protection from harmful commercial practices to the local implementation of evidence-based practices, as described

































{kind=link}