WBTi UK Steering Group members, Helen, Clare, Alison and Patricia, were very pleased to be invited to give a presentation on the 2024 Report to the All-Party Parliamentary Group (APPG) on Infant Feeding on 18 June, 2025. This APPG, an informal cross-party group, is hosted by Liberal Democrat MP for Chichester, Jess Brown-Fuller, who is a staunch advocate for breastfeeding. Meetings are quarterly.
(left to right) Jess Brown-Fuller MP, Helen and Patricia during the presentation
The hybrid event was held in Portcullis House, which is close to the Houses of Parliament and overlooks the River Thames.
At the meeting, Helen and Patricia gave an overview of the Report’s findings. This triggered a range of questions from the audience in the room and online. Attendees included Labour MP for Ribble Valley, Maya Ellis, and Liberal Democrat MP for mid-Sussex, Alison Bennett, along with representatives of Royal Colleges and local public health teams, as well as the breastfeeding support organisations.
(left to right) Jayne Joyce and Emily Lunny (LLLGB), Helen Gray and Patricia Wise (WBTi Steering Group) and Katie Pereira-Kotze (First Steps Nutrition Trust)
Presentation title slide
APPG meetings
If you would like to be notified about future Infant Feeding APPG meetings, please contact Edmund Legrave, Parliamentary Assistant for Jess Fuller-Brown: edmund.legrave@parliament.uk
Jess Brown-Fuller, MP for Chichester, hosted the formal launch of the WBTi 2024 UK report on July 24th 2025 in the Jubilee Room at the Houses of Parliament.
(left to right) Patricia Wise, Clare Meynell, Jess Brown-Fuller MP with visiting baby Niamh, Helen Gray, Alison Spiro
Kate Quilton
Investigative journalist Kate Quilton drew on her own experiences in emphasising the importance of a policy framework, and chaired the Q&A.
What do policymakers need to do, to protect and support breastfeeding?
The WBTi 2024 report made a number of key policy recommendations on maternity rights, marketing regulations and food safety.
WBTi’s ‘big ask’
The aim of the WBTi project is to galvanise action to implement report recommendations, thus improving support and protection for infant feeding. Our single most immediate actionable ask is for the UK and devolved governments to adopt the eleven recommendations of the Competition and Markets Authority (CMA) report on regulating misleading infant formula promotion. Adopting these would help to end the profiteering we have seen in recent years (formula prices have gone up by 24%! including one by 49%!). This would also help families make informed infant feeding decisions and for them to be able to access affordable products to feed their babies if needed.
The CMA recommendations encompass many of the WBTi UK recommendations on protecting families from exploitative marketing. In addition, WBTi calls for the regulations to apply to ALL formulas from 0-36 months. This would help end the loopholes that companies use in the marketing of formulas for older babies and toddlers, or for special medical purposes.
Professor Nigel Rollins
Professor Nigel Rollins, who formerly worked for the World Health Organisation and is now at Queens University, Belfast, gave a policy overview and more details about our ‘Call to Action’.
Parents are struggling
Professor Amy Brown of Swansea university stunned the room when she revealed some of the shocking findings of her research into the challenges families are facing to afford the high prices of formula.
Professor Amy Brown
Her presentation called for:
Lower priced milks – consistent, reliable and affordable pricing
Accurate information, not adverts
Parents should be supported to feed their baby without worrying about cost
For the health and well-being of parents and babies to be put before profits
She shared powerful testimony about the impact of the high cost of formula from parents themselves:
Breastfeeding is important
“Breastfeeding is a human right for both mother and child” (UN human rights joint statement 2016).
WBTi work is built on a foundation of human rights. UN human rights experts have made it clear that breastfeeding is a right of the dyad, the mother and infant together. The rights of one don’t supercede the other; mother and baby have rights as a dyad. It is the responsibility of our governments to support and protect those rights, by providing skilled health care, maternity protection at work, and protecting the rights of women and families to make their own informed decisions about how to feed their baby, without commercial influence.
What is the impact of low breastfeeding rates in the UK?
High costs for the NHS:
Low UK breastfeeding rates are costing the NHS £millions:
54,000 more GP appointments
9,500+ additional hospitalisations
Research has shown that basic interventions to support more mothers to breastfeed for longer could pay for themselves within a year. (Renfrew et al 2012)
Costing our planet:
The formula and dairy industries have a significant footprint both of greenhouse gases and water.
“For the UK alone, carbon emission savings gained by supporting mothers to breastfeeding would equate to taking between 50,000 and 77,500 cars off the road each year” (Joffe et al 2019)
Key recommendations from the WBTi Core Group
Our governments must address the ‘baby blind spots’ in national policies:
Protect all infants by adopting in full the recommendations of the CMA, and extending the regulations to cover all infant milks up to 3 years, in order to address current loopholes in marketing formulas for older infants or for special medical purposes.
WBTi recommends that regulations on safety and on marketing should be applied to feeding equipment such as bottles, teats, and other equipment, as well.
Protect infants and young children in emergencies by developing guidance on their care.
Protect the health and the rights of women and children by providing statutory rights for flexible breastfeeding/ expressing breaks and suitable facilities in the workplace and in education.
Develop a national infant feeding strategy and leadership for England.
Improve monitoring and evaluation by strengthening and coordinating data collection systems.
Helen is a member of the Steering Group for the World Breastfeeding Trends Initiative (WBTi) project in the UK.
An IBCLC and La Leche League Leader (breastfeeding counsellor), she has served as both Communications Co-Chair and Policy and Advocacy Lead for Lactation Consultants of Great Britain. She represents La Leche League of Great Britain on the UK Baby Feeding Law Group (BFLG), which works to bring the International Code of Marketing of Breastmilk Substitutes into UK law.
Helen’s background in anthropology and human evolution has influenced her interest in how breastfeeding and the way we nurture our babies are influenced by both human biology and culture.
She is currently doing a research degree on the need for strong policies to protect infant feeding in emergencies. She has written several articles and chapters on the subject and served on the Advisory Panel for a London Food Resilience research project. She now represents BFLG on the global Infant Feeding in Emergencies Core Group.
Do YOU want to be part of driving change for our children’s future?
The second assessment is now underway. It will run throughout this year and be launched in 2024.
What is the WBTi?
The World Breastfeeding Trends Initiative (WBTi) is a human rights-based, evidence-informed, collaborative and participatory national assessment of the implementation of key policies and programmes from the WHO’s Global Strategy for Infant and Young Child Feeding, and is a project developed by the International Baby Food Action Network (IBFAN). Currently nearly 100 countries are taking part.
WBTIIndicators of Policy and Programmes
National policy, programme, and coordination
Baby Friendly Initiative
International Code of Marketing of Breastmilk Substitutes
Maternity protection in the workplace
Health professional training
Community based support
Information support and communications
Infant feeding and HIV
Infant and young child feeding during emergencies
Monitoring and evaluation
In 2016, the UK scored just 50.5/ 100 on these ten key policy indicators.
WBTi brings together the main government agencies, health professional bodies, and civil society organisations involved in infant and maternal health and nutrition in each country to work together to collect information, identify gaps and generate recommendations for action. This Core Group must be free of conflicts of interest from the baby feeding industry (all infant or toddler milks up to 3 years, baby foods, bottles or teats).
The Global Breastfeeding Collective, led by WHO and UNICEF, recommend that the WBTi process be repeated, at least every 5 years, to monitor implementation of key policies, and include this in each country’s score on the Global Breastfeeding Scorecard.
Volunteers wanted
Many volunteers contributed to the success of the first UK WBTI assessment in 2016.
Your contribution is valuable, large or small:
Writing
Social media
Graphic design
Advocacy
Freedom of Information requests.
Fundraising
Mapping infant feeding training standards
Auditing numbers of breastfeeding counsellors and peer supporters
Project management
Virtual assistant skills
Parliamentary research
and more
You can find the main WBTi UK 2016 Report Part 1, and Part 2 with supplementary material, with Report Cards for each of the four nations and for the UK overall, here: https://ukbreastfeeding.org/wbtiuk2016/
Our WBTi work has revealed that in the UK we have no national guidance on the support and feeding of infants and young children, or pregnant or breastfeeding mothers, during emergencies. There is currently a postcode lottery of Local Resilience Forums who include a few details in their advice to the public such as “Remember to pack formula and nappies for your baby”, but there is no national guidance for LRFs and local authorities that they should include infants and young children in their planning.
This page will serve as a repository for resources for those planning services and those providing feeding support for Ukrainian families with infants and young children.
Breastfeeding provides infants with food security, immune protection, and emotional comfort during disasters. Basic priorities in an emergency:
1) Support new mothers to hold their babies skin to skin and begin breastfeeding within the first hour.
2) Support mothers who are breastfeeding, partially or fully breastfeeding, to continue breastfeeding and increase their milk supply if needed: provide access to skilled feeding support.
3) Protect infants who are not breastfed: Trained infant feeding / nutrition support teams from trusted NGOs like UNICEF will provide access to safe supplies of appropriate infant formula for babies that need it, and support with safe preparation under hazardous conditions.
4) Protect all infants: breastmilk substitutes and feeding equipment (infant formulas and other milks, bottles, teats, breast pumps and also donor human milk) will be provided by trusted NGOs like UNICEF; the public should AVOID sending donations of these into high risk settings, but send donations of funds to trusted NGOS instead. This will enable them to provide families with what is needed on the ground.
These organisations are members of the Infant Feeding in Emergencies Core Group and have created the international Operational Guidance on Infant Feeding in Emergencies. Please consider supporting their work with families with infants and young children.
We have collected links to infant feeding resources in Ukrainian, and also in the languages of countries housing refugee families, for breastfeeding helpers and aid workers in those countries.
Please send us any suggestions for additional resources
We have a few other resources not included here; please email us any enquiries.
NOTE: we will continue to add links and resources to this page, and these organisations are continuing to add further translations into more languages – please make sure that you clear your cache, or ‘refresh’ the page, each time you open any of these links to ensure that you find the most up to date page.
NOTE: We are providing these resources as a public service, but we cannot read the resources in other languages ourselves, so we cannot always vouch for the accuracy of the contents. Please have someone fluent in the language read it for you.
Guidance for helpers not trained in supporting infant feeding
This short leaflet was written for local authorities and those supporting Afghan refugee families but could be useful for those supporting Ukrainian refugees in the UK. It sets the context, lists some useful resources for parents, provides information about making up powdered infant formula correctly and describes useful actions in some possible scenarios.
Infant feeding support resources – multiple languages
Pictorial counselling cards in many languages including Russian, adapted to include COVID19 recommendations. Some are full pictorial sets, while some are simply the translation matrix.
Infant Feeding flyer for families in transit (including English, Ukrainian, Polish, Russian, updated for COVID19). Developed by the volunteer team from Infant Feeding Support for Refugee Children/ Safely Fed
Pictorial book about breastfeeding (no words) from La Leche League Netherlands. The PDF is free to use for all. Printing and sharing is allowed, as long as the original file (including credits) is unaltered. Price listed on website is for printed version.
Breastfeeding Matters – A Guide to Breastfeeding for Women and their Families (from best Start, Ontario Canada) can be downloaded free in Russian and other languages
La Leche League International: Variety of resources and infographics in infant feeding in emergencies translated into multiple languages – most are directed at mothers and parents
Please do contact us if you are interested in volunteering or have some useful resources to share!!
CONTACT: wbti@ukbreastfeeding.org
Helen Gray MPhil IBCLC is Joint Coordinator of the WBTI UK Steering Team, and Policy and Advocacy Lead at Lactation Consultants of Great Britain. Her research interests include human rights and infant and young child feeding in emergencies.
The World Breastfeeding Trends Initiative (WBTi) is a tool to help countries assess their implementation of key policies and programmes. These are drawn from the WHO Global Strategy for Infant and Young Child Feeding, which was adopted by the World Health Assembly, including the UK. The first UK World Breastfeeding Trends Initiative report was published in November 2016 and launched at the Houses of Parliament. Its ten policy and practice indicators address the extent to which there is an infrastructure in a country to support breastfeeding. The process brought together organisations and agencies working in maternal and infant health to monitor progress, identify gaps and generate joint recommendations for action to address those gaps.
What is Indicator 1 about?
Indicator 1 asks if there is a national infant feeding policy, supported by a government programme, with a coordinating mechanism such as a national infant feeding committee and coordinator. The UK assessment found:
Women have autonomy over their own bodies so decide for themselves how to feed their babies but it can be very hard to carry a specific intention when the environment is unsupportive. It’s similar to the situation faced by someone who wants to avoid becoming overweight in an environment where tempting food is heavily advertised and easily available. A UK mother who wishes to breastfeed is likely to face barriers to achieving her goal throughout her breastfeeding journey.
National leadership
How can the situation be changed? An efficient way that can help to achieve consistency across the country is to have national leadership – a national coordinator with sufficient authority, a representative high level committee and a plan or strategy for change, as described in Indicator 1. Breastfeeding Policy Matters in 2015 highlighted the importance of this and the processes needed [1].
Scotland and Northern Ireland have national leadership in place but England does not. Yet the rhetoric is there. The 2016 government guidance from Public Health England, Health matters: giving every child the best start in life explains why the early years are so crucial [2]. It lists some of the health benefits and states that ‘creating the right environment to promote and support breastfeeding is crucial’. It highlights the importance of good maternal mental health so that the mother can be sensitive to the baby’s emotions and needs, helping the baby to develop secure attachment. Breastfeeding enhances a mother’s mental health while mothers who want to breastfeed but stop before they planned to are at greater risk of postnatal depression [3]. However, instead of increasing the support available to mothers, many support services were cut in 2016 because of reduced funds available. Such preventative services were not seen as a priority.
Freedom to choose how to feed one’s baby is valued in the UK and some people are concerned that mothers might feel pressured to breastfeed if it is encouraged. Ironically, advertising of follow on formula milks that might persuade mothers to switch from breastfeeding seems to cause less concern. Yet thousands of mothers make the often upsetting decision to stop breastfeeding before they wanted to. Where is the focus on these mothers and their suffering? Supporting breastfeeding is not about persuasion but about providing the infrastructure to enable them to continue; since some three quarters of mothers already opt to start breastfeeding, persuasion is irrelevant for them. If more mothers continued as long as they wished to, the proportion starting may well increase as expectant mothers will be less likely to hear negative messages.
Unicef UK’s widely endorsed Call to Action in 2016 included developing a national infant feeding strategy board in each nation [4]. What would a strategic plan encompass? The other WBTi indicators offer key points to include, such as Baby Friendly status being a universal goal, legislation in line with World Health Assembly recommendations, adequate protection for breastfeeding in the workplace, local support that is of high quality and integrated, and health professionals who have adequate training is supporting breastfeeding. If representatives of the four UK nations meet regularly they can also share ideas. Back in 2003 the World Health Organisation produced the Global Strategy for Infant and Young Child Feeding, which includes recommendations for national leadership, and this was followed in 2008 by the European Blueprint document [5,6]. Thus there are plenty of ideas available for developing a plan. The challenge is then implementation.
Alongside national leadership by governments, as described above, the breastfeeding support charities, relevant royal colleges and other similar professional bodies, campaigning organisations and interested individuals can both amplify calls for change and help to bring it about by collaborating. The infant feeding coalition meeting in June 2016, reinvigorating the idea of the former Breastfeeding Manifesto Coalition, demonstrated the keenness there is to work together [7]. Unicef UK’s Baby Friendly consultation on developing an inclusive Foundation provides an urgent opportunity to influence this – urgent because the deadline is 31 January 2017 [8].
Please read the consultation document and respond to the survey, thus helping to influence the future.
Also, check out our campaigning guidance for you to contact your MP and discuss issues highlighted in our report [9].
The launch at the House of Commons on 15 November of the first UK-wide World Breastfeeding Trends Initiative (WBTi) report on infant feeding policies and programmes gave some clues to which “stepping stones” along a family’s feeding journey are missing, where families are struggling to meet their own breastfeeding goals. While most mothers in the UK (around 80%) do set out to breastfeed, breastfeeding rates plummet within weeks until fewer than 1% of babies in the UK are exclusively breastfed at 6 months.
MPs from across the political spectrum attended the parliamentary launch, hosted by Alison Thewliss MP, along with guests from Unicef UK Baby Friendly Initiative (who provided a screening of their new short video on their Call to Action) health professional bodies, voluntary organisations, breastfeeding experts and academic researchers. Nearly 20 organisations were involved in developing the report’s recommendations for action.
These recommendations cover the family’s whole feeding journey, and range from the fundamental importance of full Unicef UK Baby Friendly accreditation of maternity settings, to health professional training and access to skilled breastfeeding support in the community, all the way to maternity protection and the provision of breastfeeding breaks in the workplace.
Dr Amy Brown gave a keynote address demonstrating how the structure of joined up policies and programmes forms essential underpinning to the cultural change that is badly needed in the UK.
Lack of political and national leadership, uneven health professional training, formula milk marketing, poor data collection and patchy community support for mothers were identified as gaps in UK policies and programmes. The degree of variability in the minimum standards of training in infant and young child feeding training among different health professions – even those working most closely with mothers and infants – was surprising.
Eyebrows were also raised at finding that, while there is guidance on the care of zoo and circus animals in case of emergency or disaster, there is no national guidance for the care of mothers and babies in an emergency situation. Formula-fed babies would be at particular risk if access to clean water and electricity were interrupted, and it is vital that national guidance be communicated to all local authorities and emergency responders.
Scotland and Northern Ireland were found to have strong strategies and national leadership in place, but England and Wales fell short.
Alison Thewliss MP, chair of the All Party Parliamentary Group on Infant Feeding, hands the new WBTi UK Report to Nicola Blackwood MP, the Minister for Public Health
The Unicef UK Baby Friendly Initiative, however, was singled out as a “world leader” in its commitment to children’s rights and for the excellence of its training programmes, both in hospital settings and in the NICU and community.
The report provides the first broad-based assessment of the UK’s implementation of ten key policies and programmes to support women and babies during their feeding journey. The policies are drawn from the World Health Organisation’s (WHO) Global Strategy for Infant and Young Child Feeding, which the UK has endorsed since 2003.
Some of the recommendations from the WBTi Core Group were actions that MPs could lead on, including the full implementation in UK law the International Code of Marketing of Breastmilk Substitutes as well as its full enforcement, and the protection of breaks for breastfeeding or expressing milk for mothers returning to work. Recent studies from Save the Children and WHO have also shown that political will is pivotal in driving forward improvement in key strategies across the board to support infant feeding.
One of the key drivers for the WBTi project in the UK is women’s choices. Although the majority of mothers in the UK want to breastfeed, many of them are struggling. The majority of these mothers wanted to breastfeed for longer but did not get the support they needed to meet their goals. Mothers who stop breastfeeding early due to unresolved problems have double the risk of postnatal depression.
The impact of infant feeding on child and maternal health is well documented, but the impact on the national economy is less well understood. In addition to costing the NHS more than £40 million for five common diseases alone, the long-term impact of the UK’s low breastfeeding rates on cognitive ability, human capital and productivity across the whole population is estimated to cost the economy at least 0.53% of gross national income.
Breastfeeding rates in the UK are lowest in its most-deprived communities, exacerbating health inequalities. Breastfeeding could prove to be a powerful means of combating inequality.
This first WBTi UK report provides a road map for policy makers and commissioners to target gaps in order to provide families with the support they need all the way through their feeding journey.
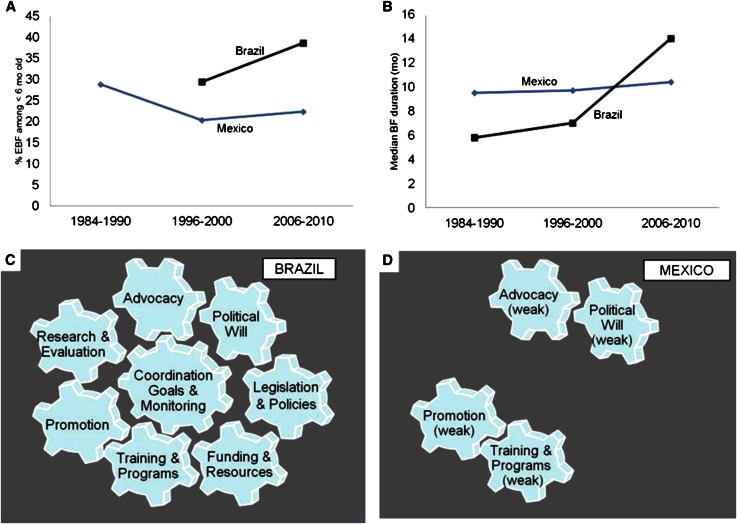
In the first presentation, this graphic popped up, and a collective “ooh” and then an “aah” went round the room. You may be forgiven for wondering why it generated such a response – it doesn’t look particularly inspiring!
Credit: Pérez-Escamilla et al, Advances in Nutrition, Nov 2012
It’s because this picture demonstrates what happens when there is a strong national strategy on breastfeeding – and also what happens when there isn’t.
In the late 1990s, Brazil made a concerted effort to improve infant health through a drive to increase breastfeeding rates in the country. They put in place legislation to protect mothers, training for health professionals, breastfeeding promotion – along with the money to pay for it all. And they had a national coordinated breastfeeding strategy to make it happen.
At the same time, Mexico had no such national strategy. Half-hearted efforts were made in some areas, such as training for health professionals and public promotion of breastfeeding.
As the graphs show, Brazil was able to significantly increase breastfeeding rates over that period while in Mexico they stagnated.
Without a strong, national, coordinated breastfeeding strategy to drive things forward, everything else is just wheels turning in the wind.
That’s the metaphor – what does this all mean in practice for the UK?
Let’s imagine a mother, who has her baby in a Baby Friendly hospital [1] and breastfeeding gets off to a good start. But then she arrives home and starts to experience some problems. Her health visitor suggests she gives the baby some formula [2]. She’s seen some adverts on television and buys a particular brand of formula because it’s “closer to breastmilk” [3]. She lives in a rural area, and the nearest breastfeeding support group is 10 miles away and she doesn’t drive [4]. Her husband has seen the adverts too so he knows that “good dads do the night feeds” [5]. After a couple of weeks the baby is getting more and more formula and is breastfeeding less and less. Her husband suggests she’s given breastfeeding a good go but maybe she should stop now [7]. She had wanted to breastfeed for longer but she gives up [8].
Indicator 2 of the WBTi asks – are babies born in Baby Friendly hospitals?
Indicator 5 asks – do health professionals have adequate breastfeeding training?
Indicator 3 asks – is the International Code of Marketing of Breastmilk Substitutes fully implemented?
Indicator 6 asks– do all mothers have access to breastfeeding support in the community?
(see Indicator 3)
Indicator 7 asks – do parents have access to good information about breastfeeding and the risks of using formula?
Indicator 12 asks – what percentage of babies are exclusively breastfed for the first six months?
Without this central cog (Indicator 1) driving all the other cogs (Indicators 2-10) things cannot move forward. This point is also made clear in a new report from Save the Children, which looked at breastfeeding policies and practices in six countries, including the UK.
there needs to be a National Breastfeeding Committee
that committee must meet on a regular basis to review progress
that committee needs to link effectively with public health bodies
that committee must have a coordinator who communicates national policy at regional and local levels
Indicator 1 of the WBTi assessment asks whether a country has each of the above and gives a total score out of 10. How well do you think the UK as whole will score? How would the countries of the UK score individually? What do we need to do to improve that score? How can policies be turned into actions at a local level?
In the next blog post we will be talking about Indicator 2 – Baby Friendly care and Baby-Friendly Hospital Initiative and will be asking for your thoughts about how things can be improved.
Don’t be fooled by the uninspiring acronym – the WBTi is the most exciting thing to happen in breastfeeding in the UK for years!
The name stands for the World Breastfeeding Trends initiative and it was launched in 2005 by IBFAN, and the idea is to take a snapshot of breastfeeding in a country – the policies, practices and breastfeeding rates – and then (and this is the important bit) to create some recommended actions to improve things.
The assessment is then repeated 3 to 5 years later and a new set of recommendations are made. The idea is to create an upward trend of continuing improvements over time so that more babies are breastfed and for longer, improving infant and maternal health.
Governments don’t need to keep reinventing the wheel because we already know what works. Back in 2003 the WHO produced (and member countries signed up for) the excellent Global Strategy on Infant and Young Child Feeding, which outlines exactly what they need to do to improve breastfeeding rates. It says that:
· All governments should develop and implement a comprehensive policy on infant and young child feeding.
· All mothers should have access to skilled support to initiate and sustain exclusive breastfeeding for 6 months and ensure the timely introduction of adequate and safe complementary foods with continued breastfeeding up to two years or beyond.
· Health workers should be empowered to provide effective feeding counselling, and their services be extended in the community by trained lay or peer counsellors.
· Governments should review progress in national implementation of the International Code of Marketing of Breast-milk Substitutes, and consider new legislation or additional measures as needed to protect families from adverse commercial influences.
· Governments should enact imaginative legislation protecting the breastfeeding rights of working women and establishing means for its enforcement in accordance with international labour standards.
The WBTi breaks down the Global Strategy into 10 areas (indicators) and asks a short set of pertinent questions to see how the country is doing in each one. Where gaps are identified, recommendations are put forward to fill them.
Studies show that countries that have enacted the Global Strategy – in all 10 areas, not just a select few – have seen great improvements in their breastfeeding rates.
Over 100 countries are involved in the WBTi but this is the first time for the UK. The beauty of the process is that it is a collaborative effort between government officials and organisations involved in breastfeeding. If you are a mother, peer supporter, midwife, health visitor or lactation consultant – we’d also like to get your views. Over the coming days we’ll be posting a key question for each Indicator and will be asking what actions you think the WBTi should recommend in its report. So stay posted…