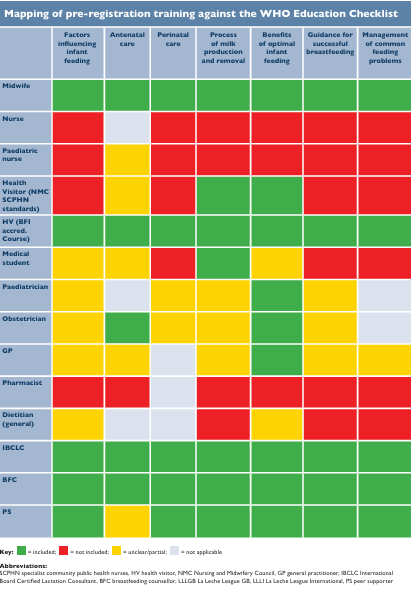

Our WBTi joint recommendations on health professional training were launched at Guy’s Hospital, London, in March 2025. The launch of our joint recommendations on policy actions, at the Houses of Parliament, followed in June.
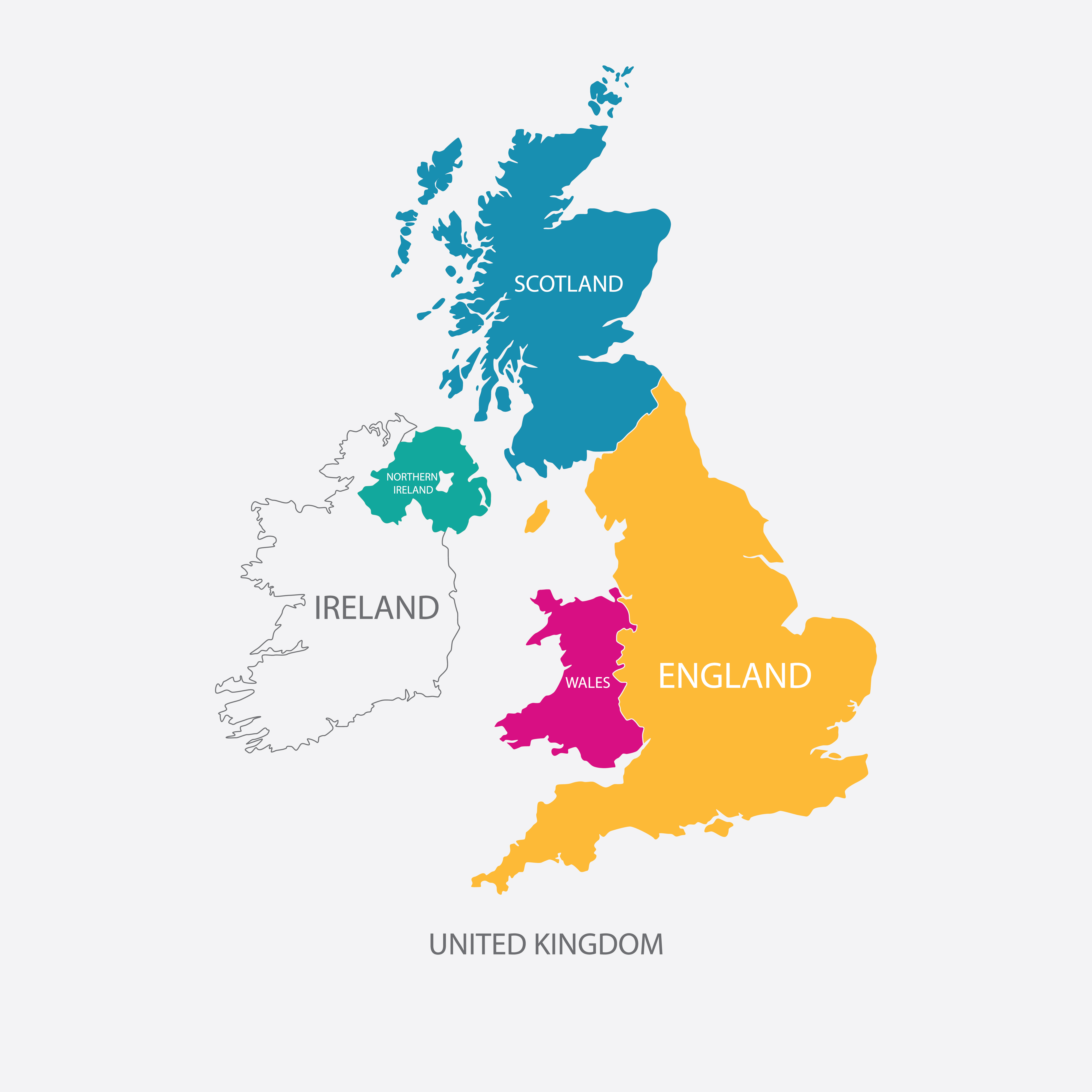
What has changed since then? Below are some of the headline data available online or sent to us from the four nations of the UK. They show progress made by the nations in addressing some of our recommendations. Although health is devolved to the individual nations, there is some collaboration between the national departments of health. An example of a difference between the devolved health systems is the variation in the ages at which infant feeding data are collected.
Our WBTi 2024 Report recommends that all nations have a comprehensive, long-term, resourced strategy to help prioritise infant feeding. This blog focusses mainly on the national strategies and breastfeeding rates.
Courtesy: Shutterstock
England
Policy and guidance
In July 2025, the Department for Education published a broad strategy for infants and children, ‘Giving every child the best start in life’, which aims to simplify and improve the early years system. It is based on the evidence that integrated early years services can significantly benefit children’s lives in wide-ranging and long-lasting ways. £900m is being invested to ‘deliver a more connected, prevention-led system that improves outcomes for babies, children and their families. Services for the early years will be provided through a network of up to 1,000 Best Start Family Hubs across every local authority in England by 2028’ (DHSC personal communication).
This broad strategy does not address infant feeding directly. In March 2026, updated guidance focussed on infants and their families, ‘Best Start Family Hubs and Healthy Babies – Preparing for implementation April 2026′, was published jointly by the Department for Education and the Department for Health and Social Care (DHSC). Infant feeding is explicitly mentioned in this guidance (pp7,11,13,16). Start for Life was renamed as Healthy Babies so Family Hubs services for 0 to 5 year olds are now called Healthy Babies services.
75 local authorities with high levels of deprivation were previously funded for 3 years (2022-2025) to set up family hubs to deliver core services in perinatal mental health, parent-infant relationships and infant feeding. £50m was ring-fenced for infant feeding. £200m is being invested in these local authorities for 2026-29, of which £55m is specifically for infant feeding. Uses of the funding are to include upskilling the workforce, peer support services and joined-up services with clear referral pathways. Alongside the Family Hubs’ services, there is also continued investment in the National Breastfeeding Helpline and the Best Start in Life website (DHSC personal communication).
In March 2026, Sharon Hodgson MP was appointed Parliamentary Under-Secretary of State for Public Health and Prevention in DHSC and her portfolio includes Healthy Babies.
The Healthy Child Programme (HCP)
The HCP is the national framework for improving the health and wellbeing of children and young people. The update, launched in February 2026, provides refreshed delivery and commissioning guidance to improve consistency in public health nursing for children aged 0–19.
It focuses on early intervention, including mental health, obesity, and parenting support via health visitors (HV) and school nurses; it also ‘reaffirms breastfeeding as a public health priority, with High Impact Area 3 emphasising the role of health visiting in delivering consistent, evidence‑based feeding support from pregnancy through the postnatal period, particularly for families experiencing inequalities (DHSC personal communication).

The HCP includes guidance at a community level, not just for individual HVs, and this covers partnership working, breastfeeding-friendly environments, implementing Baby Friendly standards and adherence to the WHO International Code.
Five face-to-face contacts are standard for all families (Universal-level offer) but extra support may be offered based on need (targeted and specialist-level offers). These contacts are health and development reviews, intended to be delivered by health visitors. There is guidance for health visiting on the high-impact areas (ages 0 to 5), including supporting breastfeeding. There is also guidance on data collection, including infant feeding.
With regard to funding, ‘Over the next three years, more than £13.4 billion will be provided to local authorities to fund public health services in England through the ring-fenced Public Health Grant, including for health visiting and family nurse services delivered through the Healthy Child Programme’ (DHSC personal communication).
Postnatal care toolkit
In January 2026, NHS England published a toolkit for integrated care boards to improve postnatal care, which is defined as the first 6-8 weeks after birth. The toolkit is intended to strengthen how services work together to achieve the standards of NICE guideline 194 on postnatal care.
A recommendation (3.2) is to improve training for health professionals, including in infant feeding/ breastfeeding support, but no specific standards are given.
Breastfeeding rates (from data collected routinely for DHSC)
The continuation rate at 6-8 weeks for any breastfeeding in England has improved since the 2024 WBTi Report was published. Rates vary with deprivation; in 2023-4, the rate in the most deprived areas was 59.1% and in the least deprived 81.3%.
The WBTi Report (hyperlink) recommended collecting data on infant feeding at various additional ages (10-14days, 6 months, 2 months and 2 years) but there is still no routine collection beyond 6-8 weeks. However, the results of the 2024 England Infant Feeding Survey were published on 4 June and these include later ages.
| % Any breastfeeding | ||
| Year | ||
| Age data collected | 2024-2025 | 2023-24 |
| Baby’s first feed breastmilk | More recent data not available | 71.8 |
| 6-8 weeks (any breastfeeding) | 55.6 | 52.7 |
Data page: https://fingertips.phe.org.uk/profile/child-health-profiles/data#page/1/ati/15
Page showing trends over time: https://fingertips.phe.org.uk/profile/child-health-profiles/data#page/4/gid/1938133228/pat/159/par/K02000001/ati/15/are/E92000001/iid/93932/age/309/sex/4/cat/-1/ctp/-1/yrr/1/cid/4/tbm/1/page-options/tre-do-1
Northern Ireland
Policy and guidance
The Northern Ireland Breastfeeding Strategy ended in 2024. The strategy review found that considerable progress had been made in several aspects, in which the work is now embedded as standard practice in many organisations involved with the strategy. Key priority areas identified by the strategy will be addressed via a new N.I. Breastfeeding Action Plan. A consultation with stakeholders on the draft action plan was held in the summer of 2025 and it is anticipated that the finalised version will be published by summer 2026.
Due to the current financial constraints, there are no resources to fund independent research, such as gathering qualitative data on women’s experiences (recommended in the WBTi Report), but the Department of Health is working with the Republic of Ireland through the All-Island Breastfeeding Policy Network to identify opportunities for learning and research. The Public Health Agency (PHA) is also exploring research opportunities in collaboration with local universities.
Breastfeeding rates
There have been gradual increases since publication of the 2024 WBTi Report (2021/22 data used), as the most recent data available (2023) demonstrates in the tables below.
| Data collection point | Year (infant year of birth) | |
| 2023 | 2022 | |
| Breastfeeding attempted | 62.7% | 62.2% |
| % Any breastfeeding: total (% in brackets)*+ partial** | ||
| Data collection point | Year (infant year of birth) | |
| 2023 | 2021 | |
| Discharge from hospital | 50.9 (33.9) | 50.8 (35.5) |
| First visit (10 -14 days) | 45.6 (32.1) | 43.0 (31.6) |
| 6-8 weeks | 37.2 (26.5) | 34.6 (26.0) |
| 3 months (14-16 weeks) | 31.3 (23.3) | 29.3 (22.4) |
| 6-9 months | 24.7 (18.6) | 22.4 (17.3) |
| 1 year (12-14 months) | 16.7 (12.1) | 11.3 (8.4) |
*Total breastfeeding=fed only breastmilk, both at the breast and expressed.
**Partial breastfeeding=fed breastmilk and other milk.
Data for 2023 supplied by PHA Health Intelligence, March 2026:
- Breastfeeding attempted – Northern Ireland Maternity System (NIMATS); Live births to Northern Ireland resident mothers; excludes home births, free births and infants who died in the delivery suite. Note: Data presented for 2023 is based on NIMATS data but excludes births in South Eastern HSCT following transfer to EPIC on 9 November 2023.
- Discharge to 12 months – Northern Ireland Child Health System (NICHS); Live births to Northern Ireland resident mothers. Data will include resident mothers who gave birth outside Northern Ireland. Note: Discharge data for 2023 will include births recorded on EPIC to mothers resident in the SEHSCT area which impacts data quality and recording.
Encompass/EPIC is a new electronic patient record system that will create a single digital care record for every citizen in Northern Ireland who receives health and social care. It aims to create better experiences for patients, service users and staff by bringing together information from various existing systems. The programme was launched in the South Eastern Health and Social Care Trust (HSCT) on 9 November 2023. The system also went live in Belfast HSCT on 6 June 2024, and Northern HSCT on 7 November 2024 with roll out to Southern and Western HSCTs on 8 May 2025.
Data used by WBTi for 2021/2022 available from the PHA Health Intelligence Briefing
Scotland
Policy and guidance
The Scottish government launched a new strategy, Breastfeeding and infant feeding: strategic framework 2025-2030, in June 2025. It sets out how it will ‘further implement recommendations from the 2019 Becoming Breastfeeding Friendly report, and integrate them into broader action including responding to the World Breastfeeding Trends Initiative (2024) report card for Scotland.’ The UN Convention on the Rights of the Child (CRC) is now embedded in Scottish law and the CRC Committee’s 2023 recommendations include strengthening breastfeeding support for mothers, implementing the WHO Code and raising awareness of the importance of breastfeeding among the general public.

In November 2025, the Scottish government refreshed its stretch aim to reduce the drop-off in breastfeeding rates at 6-8 weeks and it is now a 10% reduction by 2031. The rate of drop-off has reduced from 34.5% in 2017-18, when the stretch aim was announced, to 25.3% in 2024-25.
An annual update on progress will be provided in the coming months, together with a forward look.
As of 2025/26, 85% of neonatal units are Baby Friendly accredited. Other services are 100% accredited: maternity units (achieved 2015), community trusts (2018) and universities (2021).
For staff training, there is a permanent national programme lead, and various resources. Breastfeeding is included in the national curriculum for secondary schools (section 2.3.7).
Breastfeeding rates
The rate of any breastfeeding at 6-8 weeks in Scotland has increased steadily over the past 10 years, from less than 40% to 49% (2023-34), more so among groups that traditionally did not breastfeed, thus helping to reduce inequalities.
The 2016 WBTi Report recommended routine data collection beyond 6-8 weeks, which the Scottish government was then considering, and later implemented.
| % Any breastfeeding (% excl.*) | ||
| Year | ||
| Age data collected | 2024-25 | 2023-24 |
| Birth (ever breastfed) | 69 | 66 |
| 10-14 days | 61 (39) | 59 (38) |
| 6-8 weeks | 51 (34) | 49 (33) |
| 13-15 months | 22% (10% excl for milk feeds) | 21% (10% excl for milk feeds) |
Data are from the financial years:
2024-25 https://publichealthscotland.scot/media/35987/2025-11-11-infant-feeding-statistics-report-final.pdf
2023-24 https://publichealthscotland.scot/media/29816/2024-11-12-infant-feeding-statistics_report.pdf
* Figures in brackets are for exclusive breastfeeding. At 13-15months, this means 10% were receiving only breastmilk for their milk feeds.
Wales
Policy and guidance
Our 2016 Report recommended having a high-level funded specialist lead, and the role of National Breastfeeding Lead Midwife at Public Health Wales was recently made a permanent position.
There is a 2025-27 delivery plan for helping prevent and reduce obesity which includes a section on infant feeding and encouraging breastfeeding. An action is to develop and deliver a new feeding action plan, replacing the 2019-2024 plan.
A recent assessment of maternity and neonatal services, published in February 2026 recommends ‘that the Welsh Government requires all maternity, neonatal and relevant education providers to actively progress through the stages of UNICEF UK Baby Friendly Initiative accreditation’ (p.129). This aligns with the WBTi report recommendation to implement and maintain Baby Friendly standards across all health boards in Wales.
The digital data system, BadgerNet, replacing hand-held notes, is being rolled out across Wales and the national dataset it will cover has been agreed. The WBTi Report recommended that Public Health Wales and Health Boards work together to improve the collection of data.
Breastfeeding rates
Rates of any breastfeeding continued their gradual rise at all ages where collected (birth, 10 days, 6 weeks, 6 months).
| % Any breastfeeding (% excl.) | ||
| Year | ||
| Age data collected | 2025 | 2023 |
| Birth | 66 | 65.2 |
| 10 days | 60.7 | 55.4(37.9) |
| 6 weeks | 49.2 | 40.7(29.1) |
| 6 months | 35 | (20.9) |
Note: exclusive breastfeeding rates in brackets; 2025 Welsh data are for July-Sept.
Conclusion
The devolved nations vary in their progress towards having a current infant feeding strategy. England has taken a different route, with a broad strategy for infants and children and accompanying guidance covering infant feeding.
Data collection is a key foundation for governments to monitor quality improvement, and to help target resources. The four nations collect data at different ages, making comparison between them difficult. England still does not collect data routinely beyond 6-8 weeks but does now have the survey results.
All the nations have made some progress in line with recommendations in the WBTi UK Report and shown improvements in breastfeeding rates. These are very welcome but it is essential that improvements continue as so many mothers still do not achieve their breastfeeding goals. The newly published survey for England found 72% of mothers who stopped by the time their baby was 4-6months old would have liked to continue breastfeeding for longer!

Author: Patricia Wise

Patricia Wise is an NCT Breastfeeding counsellor and a member of the WBTi UK Steering Group. She has a particular interest in health professional training in breastfeeding and her e-book, Supporting mothers who breastfeed: a guide for trainee and qualified doctors, is available on the WBTi website.