The inquiry is very keen to hear from parents about their experiences and also from those who work with families who are using infant formula. In particular, the inquiry hopes to hear from and about a wide range of people, including those involved with the Healthy Start scheme, teenage parents and refugee and homeless families.
There is a straightforward form that can be used or people can send in a description of their experiences:
The inquiry is being led by dietitian Helen Crawley of First Steps Nutrition.
Please do pass on this message to others who may be interested so that the inquiry receives a large number of responses from and about a wide range of families.
I was asked to deliver a 15-minute talk at the Institute of Health Visiting and Royal Society of Public Health conference in April, entitled: The role of the infant feeding specialist. The following is a synopsis.
I started by sharing the story of a client whose journey will sound familiar to many IBCLCs – a first time mum who gave birth in a fully accredited Baby Friendly hospital, but struggled to breastfeed from the beginning. After receiving support with skin to skin, basic positioning, hand expressing and cup feeding, the mother went home exclusively pumping and supplementing with formula. She received a lot of support from midwives, health visitors and peer supporters, but by 10 weeks had still never had a successful breastfeed.
What the mother needed was specialist breastfeeding input, which she eventually found, to resolve her complex issues, and she continues to breastfeed, exclusively, to this day.
While most mothers begin breastfeeding, the sharp decline in the number of mothers still breastfeeding is staggering in the first 2-6 weeks. Many of the problems that women encounter are basic challenges which are solvable with the correct support.
The issue is not whether most health professionals are doing a good job, but whether every mother can access the level of support that she requires. That may be “basic” infant feeding training such as BFI trained midwives and health visitors; or it may be “additional” support from a network of trained peer supporters, or in some complex cases, where the basic and additional levels of care have not solved the mothers’ problems, access to “specialist” infant feeding care may be required (see below). It is an equity issue that there is not access in every area to trained specialist care for complex cases.
Relevant guidance from NICE, PHE and BFI are summarised in this “Guide to the Guidance” from Better Breastfeeding, outlining three recommended levels of support:
1) Basic support: A universal service with health professionals with BFI standard training in infant feeding
2) Additional support: Social and trained peer support
3) Specialist support: access to a referral pathway to specialist support for complex cases.
The recommendations from the WBTi report and BFI both agree that for some mothers, access to specialist breastfeeding support should be available and readily accessible.
While most mothers only require routine care, with the adjunct of drop in groups, peer support and telephone helplines, some mothers will require a more thorough and specialised level of care in order to overcome their breastfeeding challenge and continue to breastfeed for as long as they wanted to.
The problem is how that service is provided. The BFI provide guidelines on the person specification of the Infant feeding lead . Many of these individuals are very experienced, skilled, hard-working and dedicated. But the fact remains that there is no set of core competencies, and no requirement for the infant feeding lead to have an infant feeding qualification. This makes the skill set of the infant feeding lead a vulnerability in itself .
In many cases, the infant feeding lead is required to achieve an enormous amount, encompassing audit, training, logistical management, liaising with key partners and commissioners, as well as provide a clinical service. This role is usually undertaken on a part time basis, often supplemented with countless hours of unpaid overtime in order to fulfill the requirements of the post.
Specialist infant feeding support: a team effort
For best results, infant feeding support requires a whole team
Ideally, in order to provide the best service for families, and achieve sustainability, infant feeding support should be the responsibility of a team. Appropriately trained professionals should work together to deliver a service, so that it is not the sole responsibility of one overworked individual. These teams should include medical input from paediatricians, alongside dietetic and speech and language specialist support. Health visitors, midwives, community nursery nurses, and specialist breastfeeding support from an extensively trained member of staff, such as an IBCLC or accredited breastfeeding counsellor, should also make up the team.
For women and babies with complex feeding problems, the infant feeding specialist service should be readily accessible, timely, and high quality, with a clear referral pathway as recommended by the BFI. But importantly, this service needs to seamlessly transfer families back into routine care and follow up support. This would free up the specialist service and reduce the likelihood that the other health professionals providing routine and additional care become de-skilled.
Research indicates that delayed, inaccurate and inappropriate advice can reduce maternal confidence and self-efficacy, and leads to frustration, confusion and ultimately reduces the duration and exclusivity of breastfeeding.
Specialist skills and knowledge
The value of the infant feeding specialist is that their advanced skills and training provides them with expert listening and problem-solving skills. Infant feeding specialists such as IBCLCs possess the necessary clinical skills and training to accurately assess a problem and make an individualised plan: keeping the baby fed, protecting the maternal milk supply, and ultimately tackling the underlying cause of the problem (ILCA, 2011).
Having initially trained as a paediatric nurse, and later as a health visitor, I quickly realised that to be an effective practitioner, competent and confident to take on the management of more complex breastfeeding challenges, I needed some additional training. IBCLCs are required to not only have more than 1000 clinical practice hours, but also study an extensive curriculum, to equip them to understand and support mothers and babies with a whole range of breastfeeding problems. Moreover, we are required to keep our skills and knowledge sharp by completing 15 hours of CPD in advanced lactation and ethics every year, and by resitting our exam every ten years. I have now been an IBCLC for over 7 years, and though I still feel like a ‘junior’ compared to many of my IBCLC colleagues for whom I have a great deal of respect, my training and experience has helped me to feel capable of handling both entrenched and complex breastfeeding problems, and also to be a resource for the wider healthcare team.
Faulkner and Finch’s 2016 research found that many IBCLCs already hold infant feeding lead posts, or work in the voluntary sector. Other infant feeding leads have accessed further skills and training that equips them to run a specialist service.
Challenges
However, there are challenges. Firstly, many infant feeding leads are swamped with administrative and managerial tasks which detract from their clinical and educational role. Secondly, many infant leads are working in isolation, and simply do not have any cover when they are sick, take holiday or are overloaded. Thirdly, some infant feeding leads do not have enough access to advanced training to equip them to run specialist services, or do not have the time to be able to disseminate best practice to their team. Finally, many third sector services have been cut, which leads to services becoming overwhelmed, or women simply not having anywhere to turn when challenges crop up.
A successful specialist infant feeding referral service should be free, accessible, well-resourced, seamlessly linked with routine and additional care, and multi-disciplinary. Professionals should know where to access further training and be able to signpost families to quality sources of information. IBCLCs are well-placed to run these NHS services, and in many case they already are, but a greater emphasis on training of the entire infant feeding team would strengthen the approach and ultimately make the service more sustainable.
Photo credit: Laura Pedrick
Lyndsey is an experienced Paediatric Nurse, Health Visitor, International Board Certified Lactation Consultant, Holistic Sleep Coach and Birth Trauma Recovery Practitioner, with almost 20 years experience working with infants, children and families in hospitals, clinics, and the community.
Lyndsey runs a busy practice offering one-to-one specialist breastfeeding, bottle feeding, sleep, eating, behaviour and parenting support to families in the UK and Internationally. Lyndsey is the author of Holistic Sleep Coaching and has published a number of articles in academic journals, as well as parenting magazines regarding breastfeeding, caring for premature babies and sleep issues in children. She regularly teaches health and childcare professionals, lectures as an independent speaker, and hopes to begin her PhD later this year.
The WBTi UK Report recommendations for Indicator 4 are for government action, including legislative change:
Governments to legislate for reasonable breastfeeding breaks and suitable facilities for breastfeeding/expressing in workplaces and educational institutions.
Governments to ensure that tribunal access is available to women from all income brackets.
Government agencies to monitor provision for employees.
Governments to raise the minimum rate of maternity pay and maternity allowance to the recommended minimum wage level.
I recently heard about Rose (not her real name). Rose is in her mid-twenties and breastfeeding her second baby. She found breastfeeding to be straightforward with both children. Rose planned to return to work when her second baby was 6 months old as the family needs two incomes to manage financially.
When her baby was 5 months old, Rose quickly found a highly suitable retail job, involving working some evenings and a Sunday shift. There would be no childcare costs as her husband is at home at those times.
However, induction for the job involve attending the store for the whole of one Friday. No information was given in advance about the timing of the lunch break so Rose could not arrange for her baby to be brought to her for a feed. She was very upset the evening before at the thought of being away from her baby for a whole day. Breastfeeding is a private matter for her and she felt too embarrassed to mention to her new employer that she is breastfeeding and also feared she might be seen as a difficult employee.
If employers expected that a mother with a young baby might be breastfeeding, and routinely checked whether she had any specific needs, mothers like Rose would be supported when they return to work, rather than facing additional stress and worry.
Resources
If you or someone you know needs advice on rights at work, including maternity pay and benefits, Maternity Action has information on its website and a telephone advice line:
Conference hosted by the Institute for Health Visiting and the Royal Society for Public Health, with the WBTi UK team.
10.00 Opening Remarks Chair: Dr Cheryll Adams CBE, Executive Director, Institute of Health Visiting
A public health view of breastfeeding
10.10 Breastfeeding as mother and physician – Dr Louise Santhanam, GP and Chair, the GP Infant learning from experience and learning needs Feeding Network (UK)
10.20 Why breastfeeding is important for everyone’s health Dr Russell Viner, Paediatrician and President, Royal College of Paediatrics and Child Health (from March 18)
10.40 Strengthening the public’s health from the start, what roles for the Hearts Milk Bank? – Dr Natalie Shenker, co-founder, Hearts Milk Bank
11:00 The importance of breastfeeding and early years Jonathan Ashworth MP, Shadow Secretary of State for Health
11:15 Questions
11:25 Refreshments
Strengthening breastfeeding in the UK
11.45 The WBTi findings and recommendations for the UK Helen Gray IBCLC and Clare Meynell IBCLC, Joint Coordinators, World Breastfeeding Trends Initiative (WBTi) UK
12.05 Education and training of health visitors and other health professionals through the Baby Friendly Initiative Sue Ashmore, UNICEF, Baby Friendly Initiative
12.25 The impact of breastfeeding on mental health Professor Amy Brown, Associate Professor and maternal and infant health researcher, Swansea University
12:45 Questions
13:00 Lunch
Breastfeeding in the community – what works?
Specific issues:
14:00 The importance and challenges of peer support Dr Gill Thomson, Reader & Associate Professor in Perinatal Health, MAINN, UCLAN, and Louise Hunt, PhD student
14.15 The role of the infant feeding specialist Lyndsey Hookway, Paediatric nurse, HV and IBCLC
14.30 Medway – A System Wide Strategic Approach Scott Elliott, Head of Health and Well-being Services, Public Health, Medway Council
14.45 Discussion and questions
15:00 National developments for breastfeeding Professor Viv Bennett CBE, Chief Nurse, Public Health England
15.15 Refreshments
Moving forward – national and local actions required to increase UK rates of breastfeeding
15:35 National expert opinion and panel discussion Scott Elliott, Head of Health and Wellbeing Services, Public Health, Medway Council
Shereen Fisher, CEO, The Breastfeeding Network
Emma Pickett, IBCLC
Alison Spiro, Specialist Health Visitor
16.25 Chair’s closing remarks Dr Cheryll Adams CBE
Breastfeeding: a public health priority
Thursday 19 April 2018, 9.30am-4.30pm 28 Portland Place, London W1B 1LY
Indicator 3 of a WBTi assessment is about implementation and monitoring of the World Health Assembly International Code on the Marketing of Breastmilk Substitutes. UK Regulations only partly incorporate the International Code yet the regulations still get broken, as the WBTi UK report of 2016 illustrates with examples of idealising text and images on packaging, and price reductions.
Last month, Save the Children published a report called Don’t Push It: Why the formula milk industry must clean up its act.It emphasises that breastfeeding saves lives but that millions of children are at risk form the rapid growth in the infant formula market. The report looks at the activities of six multinational companies which have more than 50% of the market between them – Abbott, Kraft Heinz, Friesland Campina, Danone, Nestlé and RB. Responses from the companies are on the charity’s website, along with its replies to them.
The market has grown very rapidly, increasing five-fold in two decades, and it is estimated will be worth more than $70 billion by 2019. The companies spend far more promoting their products than is spent by public health budgets in supporting breastfeeding. Examples of recent company marketing in the UK that contravene the International Code, and in some cases break the law as well, are described in the monitoring report, Look What They’re Doing in the UK – 2017 .
In its report, Save the Children calls on the companies to commit publicly to upholding the Internation Code to protect children’s health as well as governments incorporating the Code fully into legislation. It is also calling on investors to hold companies to account to increase their compliance, stating “Business models that undermine the health and wealth of future generations pose a long-term financial threat to investors.”
With the widespread use of IT in business, why is it that retailers do not have systems that prevent illegal marketing such as price reductions? Instead, monitoring in the UK relies on volunteers. If you do find any reductions and inform the store manager, you might also like to ask why their electronic stock control system doesn’t include information to prevent such violations.
Panama Canal (photo credit: P Wise)
I was recently on holiday in Panama and went into a couple of supermarkets, where I noticed that baby foods were labelled as suitable from 6 months. On the basis of this small sample, I then wondered whether Panama has a strong law. Indeed, the International Code is fully integrated in national law although, as the committee on the rights of the Child reported in January 2018 , there is no monitoring or sanctioning mechanism.
Once upon a time there was a town where the young people had two options available when they wanted a place of their own to start a family . They could either live in the town, in existing apartment blocks, or build their own home on the edge of the town. Some preferred the apartments because they were already built using a tried and tested construction by large companies or they had grown up in the area and would be close to friends and family who had also had the same experience and had similar views to their own.The apartments provided adequate accommodation but those who preferred to build their own home liked the fact that it was healthier to live away from the pollution of the town and they could have a garden.
Those who built their own houses found it was hard work at first as they learned the techniques of construction. Those who had known and watched other people building houses tended to find it easier than those who had not been given the opportunity to see or learn how a house was built.
Some people found professional builders who could advise them on tricky issues such as what a solid foundation looked like or guidance with more minor aspects of design. Some local builders even offered free services. Unfortunately, there was also a few rogue builders, who always charged a much higher price than the others yet gave poor advice.
General advice was offered by big construction companies who built apartments in towns throughout the land, including this town. Their information was always complimentary about self build construction but somehow always implied that young people would find it “much easier and more convenient” if they moved into an apartment.
Some young people found enough encouragement to continue with their project by knowing that other self builders were also finding it hard. Some benefited from the learning process that others had experienced and willingly shared with them during the early stages of the house building.
However, other young people were unaware there was any help available and struggled on without support. Some eventually completed their houses. Others lost confidence and decided to move into an apartment after all, especially if the building work seemed to be taking over their lives or friends and family members doubted their ability to finish. Some consoled themselves with focussing on the convenience of being close to those they knew well so could share the tasks. Others believed that the idea of building one’s own house was oversold and felt annoyed with those who had originally suggested it to them. Some felt guilty that, even though they had tried so hard to build their own house, their children would live in the more polluted town air.
Those who completed building their houses felt proud of their achievement, especially if they had overcome major difficulties at the beginning. They still had ups and downs with repairs and maintenance, but they were happy in knowing, as a result of their personal endeavours, that their children would have a healthy future. The shared feelings among the house builders helped to form a new supportive community for other house builders. However, they hesitated to mention their homes if they met someone from an apartment in case that family had suffered an unhappy experience trying to build their own house.
Although they were all citizens of the same town, mischiefmakers spread rumours that there was ill-feeling between the two groups. But then an enlightened town council was elected that realised the need for better information about all the options available for the young people. Education in building skills for those who wanted to construct their own house, with professional help available if needed, was made readily available. The council invested in these services and also improved the byelaws and monitoring, to protect the citizens by preventing the big commercial companies from disseminating misleading information and also to catch any rogue builders.
When Christmas came, all the young people of the town held a party, showing the other citizens that they had much more in common than the differences between how their homes were constructed.
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group.
On Tuesday 28th, Dr Ruth Stirton of the University of Sussex joined forces with the World Breastfeeding Trends Initiative (WBTi) Steering Group, along with Marie McGrath of the Emergency Nutrition Network, to present on the topic of safe provision for feeding infants and young children in emergencies in the UK. This WBTi UK first anniversary forum was hosted by Alison Thewliss MP, chair of the All Party Parliamentary Group on Infant Feeding and Inequalities, at the Houses of Parliament.
Participants included infant feeding specialists and policy makers, emergency planners, international academics, and third sector organisations such as UNICEF UK Baby Friendly Initiative and Save the Children.
We heard from Clare Meynell and Helen Gray (WBTi UK) on the findings, gaps and recommendations from the WBTi UK report surrounding infant feeding in emergencies. Ruth Stirton presented on the legal and regulatory framework and the minimal place of infants and young children in the current framework. Marie McGrath then described the recently published 2017 Operational Guidance on Infant Feeding in Emergencies, and explored how it might be adapted to the UK context.
The audience engaged in lively group discussion, considering:
the issues in the immediate response phase
how best to support formula feeding families in emergency situations
mapping the existing local capabilities that emergency plans could call upon
issues surrounding communication with the public and front line responders about how best to support infants and young children in emergencies
the wider policy framework and how best to ensure that infants and young children are specifically provided for
issues for the longer term recovery phase after the emergency
A report will be published in 2018 making recommendations for improvements. If you would like to contribute written comments to the report, please look at the presentations and group materials and send comments by email to Ruth Stirton r.stirton@sussex.ac.uk
WBTI Steering Group Helen Gray, Patricia Wise, Alison Spiro, (Clare Meynell in absentia), with host Alison Thewliss MP, and Dr Louise Santhamum and Dr Rosemary Marsh (GP Infant Feeding Network) and Dr Ruth Stirton (University of Sussex Law School)
It’s a year since the first WBTi UK report was launched in November 2016 at the Houses of Parliament, giving the first snapshot of the state of breastfeeding support in the UK across the indicators. The report has been used as a basis to advocate for improvements in legislation, in strategy, and in training. It has been shared with MPs, with government ministers, as well as shared widely throughout the breastfeeding community through our website.
During the year, we have hosted monthly blogs on our website, focussing on the various indicators in turn. We have an active social media planning group that publicises the WBTi findings, our blog and activities. The team have also produced numerous journal articles, posters and conference presentations in the UK and beyond. Our talented team of volunteers have also developed a video about our findings. We continue to contribute to ongoing consultations about improving health professional training in infant feeding
Policy Forum: Protecting Infants in UK Planning for Emergencies
On November 28th 2017, we will be holding a policy forum at the Houses of Parliament, in collaboration with Ruth Stirton of the University of Sussex and hosted by Alison Thewliss MP: “Protecting Infants in UK Planning for Emergencies.” This event both celebrates the anniversary of the report and aims to achieve change in Indicator 9, “Infant and young child feeding during emergencies,” which is the policy with the lowest scores across the UK. At present, there are no UK-wide or national strategies addressing the issue and it is not explicitly mentioned in local planning.
Unicef UK Baby Friendly Initiative
The jewel in the crown of breastfeeding support in the UK is the Unicef Baby Friendly Initiative. All maternity units in Scotland and Northern Ireland are accredited and most in England and Wales are working towards it. Many community NHS trusts and boards are also on the ladder towards accreditation. Some neonatal units, university midwifery and health visiting/specialist community public health nursing courses are also involved. All are helping to raise the standards of infant support provided by these health professionals.
Cuts to breastfeeding support around the country
Sadly, the WBTi assessment found that cuts in infant feeding lead posts, drop-ins and peer support programmes as well as specialist services were occurring and this has continued. For example, Blackpool’s service was decommissioned in June and the service in Kent is under threat. It appears that there is an assumption by some commissioners that health visitors can provide a sufficient service. Health visitors do have a responsibility to provide effective support with infant feeding, and should do so at statutory visits and other contacts. However, a significant number of mothers also require specialist support, which needs time as well as skill, and all mothers can benefit considerably from the social support that trained peer supporters can provide. It seems it is not well understood how challenging some breastfeeding situations are and the amount of training required to help effectively in those situations.
Ask YOUR MP to join the Call to Action!
These cuts in services for women and babies are likely to have a negative impact on Baby Friendly accreditations. Unicef UK is holding an event for MPs at the Houses of Parliament on December 5th, asking them to pledge their support for breastfeeding. How would it be if every current MP were contacted? Are you willing to contact your MP?
Are monitoring and evaluation data regularly collected and used to improved infant and young child feeding practices?
In last month’s blog Patricia Wise explained how monitoring and evaluating breastfeeding rates is the 10th and final indicator of any World Breastfeeding Trends Initiative report, including the UK one . This blog shows how the data can be used as a tool to inform decision-making, especially for commissioning services, to reduce inequalities in child health.
Public Health datasets
Public Health England Early Years Profiles allow for measures of infant health based on International Classification of Diseases codes (ICD10) to be tracked over time and compared with statistically similar areas across England. It needs local knowledge to interpret findings as you are looking for patterns, or signals, in amongst the noise of coding and other errors. Decision-making is hard when there are gaps or significant errors in the data so it is worth spending time with all involved to improve the quality of the data.
As an example, Northumbria Healthcare NHS Foundation Trust recently received the first Health Visiting Baby Friendly Achieving Sustainability Gold Award, demonstrating a long term commitment to implementing the Unicef UK Baby Friendly Initiative. The Trust is in the 4th most deprived decile (a decile is 1/10 of the population) in England (IMD2010) so a good example of what can be achieved in communities with areas of disadvantage.
In the Northumberland PHE area (which includes Northumbria NHS Trust), breastfeeding prevalence rates at 6-8 weeks have increased 2 percentage points between 2010/11 and 2014/15. Opportunities for assessing wider measures of child health from the Early Years Profiles are limited so Northumberland is unusual in having data available for gastroenteritis hospital admissions for two consecutive years. These reduced from 29 per 1,000 babies under one in 2014/15 to 19 per 1,000 in 2015/16. Other factors will also contribute but there is good evidence that breastfeeding reduces the incidence of gastroenteritis and associated NHS cost savings have been calculated .
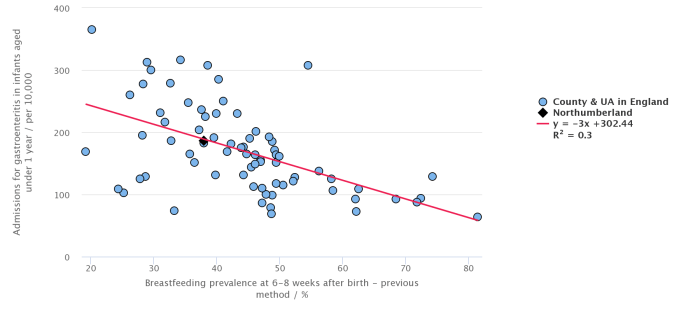
Comparing Northumberland to neighbouring trusts in the graph below, its hospital admission rate for gastroenteritis sits on the regression line. Darlington and North Tyneside have more admissions (32/1,000 and 31/1,000) while Gateshead has similar admissions to Northumberland at 20/1,000. However, all these four areas have similar breastfeeding rates. Local knowledge is key though to trying to understanding differences as South Tyneside has a low admission rate at 11/1,000 with lower breastfeeding rates.
Breastfeeding prevalence at 6-8 weeks compared with hospital admissions for infants with gastroenteritis in the North East Region
The graph on the PHE site is interactive. Comparing breastfeeding rates at 6-8 weeks with gastroenteritis rates for under 1 year olds shows the prevalence of gastroenteritis decreases as breastfeeding rates increase, as seen by the regression line. However, the variations in hospital admission rates also reduce and stabilise as the breastfeeding prevalence rates exceed approximately two thirds of the population. The reason for this is not clear. It could be an indication of a longer average duration of breastfeeding, or more exclusive breastfeeding within the population or other factors. The differences between similar communities indicate these admissions can be reduced. Since October 2015 the breastfeeding data have been obtained via interim reporting arrangements to collect health visiting activity at a local authority resident level. This new method is not comparable with the previous method so it will take some time to understand any future trends (PHE Definitions for indicator 2.02ii, Indicator ID 20202).
“In health care, geography is destiny”
Reducing these unnecessary variations in breastfeeding improves child health, helping to reduce inequalities (WBTi report p4). The impact of cuts to peer support, health visiting teams and Children’s Centres may be demonstrated within the PHE data through increasing demand for hospital services. Where children grow up influences their health.
“In health care, geography is destiny” (Wennberg, 2010).
Renfrew, MJ, Pokhrel S, et al. Preventing disease and saving resources: the potential contribution of increasing breastfeeding rates in the UK. Unicef UK BFI
Victora CG, Bahl R et al (2016) ‘Breastfeeding in the 21st century: Epidemiology, Mechanisms, and Lifelong Effect’ The Lancet Series: Breastfeeding 1 387(10017): 475–490
Indicator 10 of any World Breastfeeding Trends Initiative report is about that country’s monitoring and evaluation systems. It may not seem an exciting topic but it’s essential to collect robust data on infant feeding to know what the breastfeeding rates are and how mothers are experiencing services. Without having monitoring data how can services be evaluated and then improvements planned?
For small projects, feedback from mothers may be the most effective evaluation but for larger projects and sizeable areas, the percentages of babies being breastfed (called prevalence) at particular ages help to monitor what is happening. Figures don’t capture the ripple effect of support, though, such as a mother who’s been helped on her breastfeeding journey then supporting friends or being more likely to breastfeed a subsequent baby or deciding to train as a peer supporter.
The WBTi UK report in 2016 found that data collection and analysis had reduced considerably since the ending of the 5-yearly infant feeding survey. There is variation between the four nations with England collecting the least data.
Changing systems in England
In England, record level data on infant feeding is currently submitted by service providers to NHS Digital as part of the Maternity Services Dataset (initiation/first milk feed) and the Children andYoung People’s Health Services Dataset (6-8 weeks). Whilst these new datasets are reaching full maturity, NHS England and Public Health England are publishing official statistics on an interim basis for breastfeeding initiation and breastfeeding at 6-8 weeks respectively. Both sets of data are assembled from aggregate data submitted on a voluntary basis by service commissioners. These two breastfeeding indicators are included in the Health Improvement part of the Public Health Outcomes Framework (https://fingertips.phe.org.uk/profile/public-health-outcomes-framework).
Data on infant feeding at birth are submitted by maternity units. Babies were previously counted as breastfeeding if they went to the breast at least once in the first 48 hours. However, this is now changing to a record of the baby’s first milk feed. This is captured as part of the Maternity Services Dataset and NHS Digital publishes monthly reports on the statistics of all the indicators in the data set: as well as annual data.
Local authorities have responsibility for ensuring that their commissioned providers of the universal health visiting service submit infant feeding data for babies aged 6-8 weeks as part of the Children and Young People’s Health Services Dataset (which is about to be renamed the Community Services Dataset). As this data collection is not yet mature, aggregate infant feeding data is submitted to PHE on a quarterly basis. Official statistics are produced annually and quarterly
The Early Years part of PHOF, including these indicators, is maintained by the National Child and Maternal Health Intelligence Network.
In theory, the information at 6-8 weeks provides a picture of what is happening for the whole population but, disappointingly, there are quite a number of gaps. In most cases the local authority submits data to PHE but it cannot always be published as official statistics as a result of validation failures. This is most often due to too many records of ‘unknown’ breastfeeding status.
In one area, the health visiting service has found a solution to this by including a mandatory field on infant feeding in the electronic record of the questions about maternal mood at 6-8 weeks.
There needs to be information on at least 95% of the eligible population of babies (called coverage) to be valid and thus included. This results in some gaps in the published statistics even though the underlying data is available.
Try it yourself!
There is now a facility to compare different sets of the annual data, such as comparing gastrointestinal or respiratory infection rates with breastfeeding rates. §If there is sufficient correlation between two datasets, a red line appears. It doesn’t prove there’s a causal link though. You can try this for yourself here:
You select the Region, Area and Indicator you are interested in and then another Indicator for the Y-axis. You need to tick ‘add regression line’ to see if there is a correlation.
Using data to advocate for services
However, even if a service is well-evaluated, that does not guarantee its continued existence, as occurred with the Blackpool peer support Star Buddies programme, although this can be a useful tool in challenging actual or proposed cuts. Zoe Walsh, in her speech to Blackpool council (at 4mins 30s in the recording) in September 2017 used data as part of her clear explanation of why the service needs to be reinstated.
Data collection counts!
Cover photo credit: Paul Carter
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group.