WBTi UK Steering Group members, Helen, Clare, Alison and Patricia, were very pleased to be invited to give a presentation on the 2024 Report to the All-Party Parliamentary Group (APPG) on Infant Feeding on 18 June, 2025. This APPG, an informal cross-party group, is hosted by Liberal Democrat MP for Chichester, Jess Brown-Fuller, who is a staunch advocate for breastfeeding. Meetings are quarterly.
(left to right) Jess Brown-Fuller MP, Helen and Patricia during the presentation
The hybrid event was held in Portcullis House, which is close to the Houses of Parliament and overlooks the River Thames.
At the meeting, Helen and Patricia gave an overview of the Report’s findings. This triggered a range of questions from the audience in the room and online. Attendees included Labour MP for Ribble Valley, Maya Ellis, and Liberal Democrat MP for mid-Sussex, Alison Bennett, along with representatives of Royal Colleges and local public health teams, as well as the breastfeeding support organisations.
(left to right) Jayne Joyce and Emily Lunny (LLLGB), Helen Gray and Patricia Wise (WBTi Steering Group) and Katie Pereira-Kotze (First Steps Nutrition Trust)
Presentation title slide
APPG meetings
If you would like to be notified about future Infant Feeding APPG meetings, please contact Edmund Legrave, Parliamentary Assistant for Jess Fuller-Brown: edmund.legrave@parliament.uk
Health professional training needs to include more on infant feeding
Gaps in health professional training on infant feeding have been one of the most talked-about findings of the WBTi project in the UK.
The soft launch of the second WBTi Report on UK infant feeding policies and programmes was held at Guy’s Hospital, London, on March 25th, with a focus on gaps in pre-registration training for health professionals.
The WBTi assessment also includes in-service training. In the UK, the main source is UNICEF Baby Friendly Initiative training.
What were the gaps? Little has changed in these high level universal standards since the 2016 WBTi report. The most striking gap is that the general requirements for all nurses do not explicitly include infant feeding; this means that university health visitor training programs are not required to include much on breastfeeding, unless they are UNICEF Baby Friendly-accredited. Only 21% of university health visitor training programmes are BFI-accredited, although many health visitors will go on to receive in-service training as 69% of health visiting services in the community are now BFI- accredited. Nurses in other parts of the health system, from emergency rooms to oncology or women’s health, and even in paediatric and neonatal wards, have not routinely received training in breastfeeding.
Little support for hospitalised mothers
The WBTi team also conducted a survey of infant feeding leads on NHS Trust policies to support hospitalised mothers who are breastfeeding in wards other than maternity, for example to maintain their milk supply. We found that many Trusts lack such a policy. Scotland does have a guideline that has now been rolled out across the NHS in Scotland.
Sharing our findings
The event was well attended by key stakeholders, including representatives from the Department of Health and Social Care and devolved nations, health professional bodies, UNICEF Baby Friendly Initiative, and members of the WBTI Core Group.
The WBTi Steering Group – Helen, Clare, Alison and Patricia
Dr Bob Boyle of Imperial College set the scene with an historical background of infant feeding in the UK and globally. The WBTi team gave an overview of the report, emphasising the importance of every mother in the UK having access to an integrated network of infant feeding support, and the essential need for political commitment to enable this.
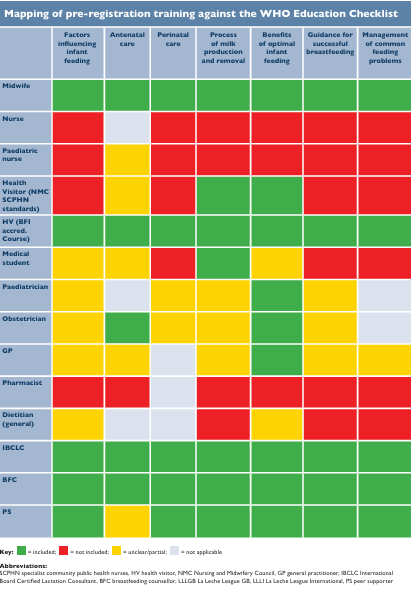
Mapping of pre-registration training standards against the WHO Education Checklist
The UK WBTI assessment maps national minimum standards for training on infant feeding topics against the Educational Checklist from WHO.
The WBTI mapping shows what any family, in any part of the UK, can expect as a minimum from their local health professionals, including not only midwives and health visitors, but also GPs, paediatricians, dietitians and pharmacists.
The assessment found some improvements, but many gaps remain, as can be seen in the chart below, with the red indicating the gaps. It is essential that everyone caring for parents have knowledge of breastfeeding. Health workers should be able to support parents’ goals, and avoid inadvertently undermining their infant feeding decisions.
WBTi summary table of breastfeeding topics in health professional standards
Table of basic standards in breastfeeding topics. More details can be found in Indicator 5 in the full report (Part 1). See Part 2 for a more detailed breakdown.
Author
Dr Alison Spiro is a member of the WBTi Steering Group. She is a retired NCT breastfeeding counsellor, specialist health visitor and hospital and community infant feeding lead, taking both trusts to Baby Friendly accreditation. She completed her MSc in 1994 and PhD in 2004 on Gujarati culture and breastfeeding, doing her fieldwork in Harrow and India.
Alison is the author of a book ‘Breastfeeding for Public Health, a guide for community health professionals’ published by Routledge.
Do YOU want to be part of driving change for our children’s future?
The second assessment is now underway. It will run throughout this year and be launched in 2024.
What is the WBTi?
The World Breastfeeding Trends Initiative (WBTi) is a human rights-based, evidence-informed, collaborative and participatory national assessment of the implementation of key policies and programmes from the WHO’s Global Strategy for Infant and Young Child Feeding, and is a project developed by the International Baby Food Action Network (IBFAN). Currently nearly 100 countries are taking part.
WBTIIndicators of Policy and Programmes
National policy, programme, and coordination
Baby Friendly Initiative
International Code of Marketing of Breastmilk Substitutes
Maternity protection in the workplace
Health professional training
Community based support
Information support and communications
Infant feeding and HIV
Infant and young child feeding during emergencies
Monitoring and evaluation
In 2016, the UK scored just 50.5/ 100 on these ten key policy indicators.
WBTi brings together the main government agencies, health professional bodies, and civil society organisations involved in infant and maternal health and nutrition in each country to work together to collect information, identify gaps and generate recommendations for action. This Core Group must be free of conflicts of interest from the baby feeding industry (all infant or toddler milks up to 3 years, baby foods, bottles or teats).
The Global Breastfeeding Collective, led by WHO and UNICEF, recommend that the WBTi process be repeated, at least every 5 years, to monitor implementation of key policies, and include this in each country’s score on the Global Breastfeeding Scorecard.
Volunteers wanted
Many volunteers contributed to the success of the first UK WBTI assessment in 2016.
Your contribution is valuable, large or small:
Writing
Social media
Graphic design
Advocacy
Freedom of Information requests.
Fundraising
Mapping infant feeding training standards
Auditing numbers of breastfeeding counsellors and peer supporters
Project management
Virtual assistant skills
Parliamentary research
and more
You can find the main WBTi UK 2016 Report Part 1, and Part 2 with supplementary material, with Report Cards for each of the four nations and for the UK overall, here: https://ukbreastfeeding.org/wbtiuk2016/
WHO and UNICEF launched the Baby Friendly Initiative (BFHI) over thirty years ago; three years later, UNICEF UK Baby Friendly Initiative (BFI) was born. The original BFHI framework of Ten Steps was created to improve maternity and hospital practices that undermined breastfeeding, such as separating mothers and their newborns or routine formula supplements, as well as implementing the International Code of Breastmilk Substitutes in maternity settings, in order to eliminate conflicts of interest with the baby feeding industry (companies that manufacture or distribute infant formula/milks, baby foods, feeding bottles and teats) such as promotion of formula milk in healthcare settings, or direct contact by companies with parents.
The Baby Friendly Initiative has changed the face of maternity practices and midwifery training in the UK – breastfeeding initiation has gone up about 20% since UNICEF UK BFI was founded in 1994. In this country, BFI has grown beyond maternity settings to create standards for infant feeding support programmes in the community and for universities training the next generation of midwives and health visitors.The BFI standards were revised in 2012, based upon the twin pillars of breastfeeding and the UN Convention on the Rights of the Child.
Routine care: all staff in the universal services (midwives, health visitors, support workers etc) are trained to BFI standard with sound, evidence-based, basic training in supporting breastfeeding and responsive infant feeding.
Additional services: every area should have additional support available, such as trained, skilled peer supporters who can act as an “informed friend” for new mothers, and a network of local peer support groups where new parents can find social support alongside help with everyday breastfeeding issues.
Specialist services: every area should also have a referral pathway for specialist care for more complex breastfeeding problems; breastfeeding specialists should have extensive experience or training such as the IBCLC qualification or a recognised breastfeeding counsellor/supporter credential, and either be a registered health professional themselves, or co-lead the specialist service with a registered health professional.
WBTi poster on Integrated Services to Support Breastfeeding, 2019
A good example of how the BFI community standards work is Harrow. Read more HERE about how WBTi UK Steering Team member and specialist health visitor Alison Spiro led Harrow’s local community health services through BFI accreditation, to develop a well integrated services and become
“the only local authority in the UK where breastfeeding was the ‘normal’ way to feed babies”
More recently, UNICEF UK BFI have produced Learning Outcomes for a wider range of health professions: medical students, paediatricians, pharmacists, paediatric/ children’s nurses, maternity support workers and nursery nurses. These will help to address the gaps in high level health professional training standards found in WBTI’s 2016 report. Every health professional who works with women, infants and children should understand the basics of lactation and breastfeeding management, prescribing during lactation, and how to refer parents on to local breastfeeding support.
#WBW2022 Webinar
On Wednesday 3 August, we will all have the chance to learn more about the Ten Steps of BFHI in a webinar produced by the Global Breastfeeding Collective, an alliance of NGOs from around the world led by WHO and UNICEF.
In addition, there will be sessions on the care of young breastfed infants who are small or with faltering growth (the MAMI Pathway) and on infant feeding in emergencies.
The entire webinar runs from 7-9 AM BST and again from 4-6 PM BST, and will be recorded.
Our WBTi work has revealed that in the UK we have no national guidance on the support and feeding of infants and young children, or pregnant or breastfeeding mothers, during emergencies. There is currently a postcode lottery of Local Resilience Forums who include a few details in their advice to the public such as “Remember to pack formula and nappies for your baby”, but there is no national guidance for LRFs and local authorities that they should include infants and young children in their planning.
This page will serve as a repository for resources for those planning services and those providing feeding support for Ukrainian families with infants and young children.
Breastfeeding provides infants with food security, immune protection, and emotional comfort during disasters. Basic priorities in an emergency:
1) Support new mothers to hold their babies skin to skin and begin breastfeeding within the first hour.
2) Support mothers who are breastfeeding, partially or fully breastfeeding, to continue breastfeeding and increase their milk supply if needed: provide access to skilled feeding support.
3) Protect infants who are not breastfed: Trained infant feeding / nutrition support teams from trusted NGOs like UNICEF will provide access to safe supplies of appropriate infant formula for babies that need it, and support with safe preparation under hazardous conditions.
4) Protect all infants: breastmilk substitutes and feeding equipment (infant formulas and other milks, bottles, teats, breast pumps and also donor human milk) will be provided by trusted NGOs like UNICEF; the public should AVOID sending donations of these into high risk settings, but send donations of funds to trusted NGOS instead. This will enable them to provide families with what is needed on the ground.
These organisations are members of the Infant Feeding in Emergencies Core Group and have created the international Operational Guidance on Infant Feeding in Emergencies. Please consider supporting their work with families with infants and young children.
We have collected links to infant feeding resources in Ukrainian, and also in the languages of countries housing refugee families, for breastfeeding helpers and aid workers in those countries.
Please send us any suggestions for additional resources
We have a few other resources not included here; please email us any enquiries.
NOTE: we will continue to add links and resources to this page, and these organisations are continuing to add further translations into more languages – please make sure that you clear your cache, or ‘refresh’ the page, each time you open any of these links to ensure that you find the most up to date page.
NOTE: We are providing these resources as a public service, but we cannot read the resources in other languages ourselves, so we cannot always vouch for the accuracy of the contents. Please have someone fluent in the language read it for you.
Guidance for helpers not trained in supporting infant feeding
This short leaflet was written for local authorities and those supporting Afghan refugee families but could be useful for those supporting Ukrainian refugees in the UK. It sets the context, lists some useful resources for parents, provides information about making up powdered infant formula correctly and describes useful actions in some possible scenarios.
Infant feeding support resources – multiple languages
Pictorial counselling cards in many languages including Russian, adapted to include COVID19 recommendations. Some are full pictorial sets, while some are simply the translation matrix.
Infant Feeding flyer for families in transit (including English, Ukrainian, Polish, Russian, updated for COVID19). Developed by the volunteer team from Infant Feeding Support for Refugee Children/ Safely Fed
Pictorial book about breastfeeding (no words) from La Leche League Netherlands. The PDF is free to use for all. Printing and sharing is allowed, as long as the original file (including credits) is unaltered. Price listed on website is for printed version.
Breastfeeding Matters – A Guide to Breastfeeding for Women and their Families (from best Start, Ontario Canada) can be downloaded free in Russian and other languages
La Leche League International: Variety of resources and infographics in infant feeding in emergencies translated into multiple languages – most are directed at mothers and parents
Please do contact us if you are interested in volunteering or have some useful resources to share!!
CONTACT: wbti@ukbreastfeeding.org
Helen Gray MPhil IBCLC is Joint Coordinator of the WBTI UK Steering Team, and Policy and Advocacy Lead at Lactation Consultants of Great Britain. Her research interests include human rights and infant and young child feeding in emergencies.
If you attended the 2015 Unicef UK Baby Friendly conference you may have noticed, or taken part, in the informal World Breastfeeding Trends Initiative (WBTi) competition to guess the final assessment score. Sue Ashfield is the winner as her estimate was closest to the actual score of 50.5 out of 100 for Indicators 1-10.
The score is a measure of how the UK is performing against the implementation of key policies and programmes to support mothers who want to breastfeed and the healthcare professionals who help them.
Sue is the lead and Specialist Health Visitor (Infant Nutrition) of First Community Health and Care in East Surrey. Sue is a winner in a much bigger way than the WBTi competition because her community team was reaccredited by Baby Friendly earlier this year and they also supported 10 local children centres in achieving full BFI accreditation in one year. The formal presentation of the award was on March 14th. Sue pays tribute to the hard work of her colleagues for the achievement but it also reflects her commitment and leadership. Read more here.
Her team is a brilliant example of what the WBTi UK report recommends for Indicator 6 (community-based support). There is close, integrated working between 0-19 public health team, breastfeeding counsellors, peer supporters and children centres at the three Baby Cafes, which have been runnning for 10 years.
Practitioners from the 0-19 team work at the Baby Cafes on a rota basis, alongside the breastfeeding counsellor. When they see mothers at home or at drop-in clinics they encourage them to attend the Baby Cafes for social support or more specialised support or just to chat to one of the peer supporters. The breastfeeding counsellors at the Baby Cafes have now trained over 200 peer supporters and this has increased the breastfeeding knowledge and skills within the local community.
Credit: Eleanor Stock
The photo above shows Sue holding the Baby Friendly Initiative (BFI) accreditation plaque along with some members of the 0-19 team, some senior managers and their BFI Guardian. Since April, all three community services in Surrey have come together as Children and Family Health Surrey to deliver children’s services.
Sue comments that she found particularly useful the information in the WBTi report about interventions and investment offered in the past and also Report Cards and the summary gaps and recommendations. She will use the findings in the report to inform local commissioners and disseminate information to staff and other stakeholders.
An integrated service like this is needed in all areas, yet in so many places services are being cut, particularly peer support programmes and breastfeeding support drop-ins.
Many congratulations Sue.
Cover photo credit: Paul Carter
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group
The inspiring story of breastfeeding support in a London borough
What changed?
I have been reflecting recently on my experiences as a specialist health visitor and infant feeding lead in an outer London borough. The story began twelve years ago, in 2005, when there was a lack of confidence among mothers and staff about the reliability of breastfeeding, which was hidden and rarely seen in public. Over the next eight years, the initiation rate increased from 67% in 2005 to 86% in 2013, and the continuation rate at 6-8 weeks from 50% to 75% (52% breastfeeding exclusively). Breastfeeding became the way most mothers fed their babies. Gradually breastfeeding mothers became visible in cafes, shopping centres, supermarkets, streets, GP surgeries and children’s centres. The Unicef Baby Friendly Initiative assessors stated in a report that, in this borough, breastfeeding had become ‘the normal way to feed babies’.
How did it happen?
How did this change come about in a relatively short period of time? It began in 2005, as a joint project between the NHS and NCT, which secured local health authority funding to set up a breastfeeding support group in an area of social deprivation with low breastfeeding rates. This group became very well attended and was facilitated effectively by two NCT breastfeeding counsellors and a health visitor. A similar group was set up in another part of the borough and was run by me, together with other health visitor colleagues. Many of the mothers were very grateful for the support they received in the groups and some of these women expressed the wish to train as volunteer peer supporters, so that they could help other mothers enjoy breastfeeding their babies, as they had. Two training courses were organised and, that year, 20 peer supporters were trained, registered by the voluntary services of the local Primary Care Trust (PCT), and started working in breastfeeding support groups, in the children’s centres and health service clinics. The news of the training spread rapidly and soon there was a waiting list of mothers wishing to train!
Reaching out
The numbers of groups expanded to be easily accessible to mothers across the borough, running every weekday, in children’s centres, cafes, and health premises. The new peer supporters brought fantastic skills with them, one setting up a website, another a mothers’ Facebook page and another designing our leaflets and posters! One had breastfed twins and set up antenatal sessions for parents expecting multiple births plus a weekly support group for mothers with twins and more. She also visited these mothers at home and lent them cushions, which helped them tandem feed. Soon the exclusive breastfeeding of twins and even triplets became common. A group of Somali mothers was trained and an outreach peer supporter started seeing Somali pregnant women in the hospital. A teenage ‘buddy’ scheme was also started by some of the younger peer supporters, working with the specialist midwife and running antenatal sessions and postnatal support for young mothers. Two peer support co-ordinators were employed to job-share this important role and to deal with concerns of the peer supporters as well as helping with training and supervision. Over the next ten years, more than 200 voluntary peer supporters were trained in the borough and the training continues until the present day.
Unicef UK/Mead
Public Health prioritises breastfeeding
In 2006, under the government scheme of “Every Child Matters’, the Director of Public Health made breastfeeding the top priority for all children in the borough with accompanying ‘stretch targets’ and funding.
London services are monitored through the ‘Good Food for London’ report on their Baby Friendly status, with details on how each borough is achieving and sustaining the Baby Friendly standards
Baby Friendly accreditation
In 2012 Unicef UK Baby Friendly Initiative carried out a major review that resulted in new, more holistic, child rights-based standards relating to the care of babies, their mothers and families, with a strong emphasis on building responsive loving relationships. A new award has also been introduced to encourage a focus on sustainability after the accreditation.
In parallel with the rapidly increasing numbers of peer supporters, the journey in the borough to become Unicef Baby Friendly (BFI) accredited started and professional training in the community and local hospital began with the two health trusts starting their journeys jointly. A model of multidisciplinary training of midwives, maternity assistants, neonatal nurses, nursery nurses and health visitors began initially with BFI-facilitated training. This enabled hospital and community staff not only to improve their breastfeeding knowledge and skills, but also each other’s roles, co-operate on work challenges and break down any barriers which may have existed previously. Communication skills and talking about their own life experiences, in order to gain an understanding of their impact, especially with infant feeding, became an important part of the in-service training. Interactive group exercises on different breastfeeding situations became an integral part of the training, emphasising the importance of empathy and seeing the problems through the eyes of the mothers. A neonatal breastfeeding co-ordinator was appointed and started training all the neonatal staff in the hospital, including the doctors, and by 2014, Unicef had awarded both the community and hospital trusts their Baby Friendly accreditation.
Peer support
Peer supporters were also employed by an adjacent borough to work in the hospital, supporting mothers on the postnatal ward, one even working all night once a week; others taught hand expressing and colostrum harvesting in the antenatal clinic, especially for mothers with diabetes.
Unicef UK/Mead
Achieving cultural change
Within ten years, breastfeeding became a normal and accepted way to feed babies in the borough. Mothers, fathers, and grandmothers-to-be came in large numbers to the twice monthly breastfeeding workshops, gaining confidence and information, with the expectation of the support that would be available to them to help them achieve their goals. A mother said ‘the session expelled myths and I now know how milk is made and transferred to my baby. I am looking forward to skin-to-skin contact after the birth and will follow my baby’s instincts’. Parents meet peer supporters in the support groups, at toddler groups, in the school grounds, in cafes, at sports events, in churches, temples, synagogues and mosques. Peer supporters live and work in the community and spread their knowledge through everyone they meet. Even when they move away from peer support, they take their embodied knowledge into the work place and support their colleagues there. Cultural change can happen through peer support, resulting in breastfeeding becoming embedded in a community. This change is sustainable over time and in future generations, as it spreads through different social groups. Voluntary peer support and informed, professional support is capable of changing attitudes and behaviour within a community to make breastfeeding ‘normal’ in a very cost-effective way. Commissioners need to be aware of how health outcomes can be improved through breastfeeding, for mothers and children, in the immediate and long-term, and it is essential to protect and increase future funding for midwives, health visitors and peer supporters, in order that vital programmes like this can continue.
The World Breastfeeding Trends Initiative UK report in 2016 affirmed the borough’s actions as it recommends in Indicator 6 (Community-based support) that ‘commissioners ensure that there is a range of postnatal services that include both health professional and voluntary-sector breastfeeding support to meet local needs and provide clear access to specialist support’ and that they ‘maintain the full range of health visiting services, and maintain health visiting as a universal service’. Indeed, the borough’s transformation in breastfeeding support is used as a case study in Part 2 of the report.
One mother with an eight-month old baby told me:
‘I so much wanted to breastfeed, but found it incredibly hard at the beginning. I was convinced that it wouldn’t work and it was such a lonely feeling, like I was failing where other mothers were succeeding. Getting support made all the difference- having someone to listen to me and give me confidence to carry on. Suddenly, I didn’t feel alone any more and it changed everything. I know that I would not be breastfeeding now if I hadn’t got help in those crucial first weeks.’
What one London borough has achieved shows what is possible. Unicef UK Baby Friendly Initiative’s Call to Action spells out four key actions to create a supportive, enabling environment for women who want to breastfeed, ranging from national strategy and legal protection from harmful commercial practices to the local implementation of evidence-based practices, as described
Will you be my Valentine? Love matters to all of us.
There will be millions of Valentine celebrations taking place all over the nation on 14 February. Hearts, red roses, chocolates, gifts, expensive treats and marriage proposals will be exchanged to signal love on that day.
But… babies are born every day. People embrace each other every day. Loving relationships begin every day! Lovers kiss every day and babies are universally loved.
Affection and love shape our brains from that first kiss on day one and continually along our life course. They create that extraordinary mother and baby bond, stimulate social interactions and enable long-lasting friendships. Early loving relationships are nurtured and supported by our families, friends, health professionals and wider society. Being held closely, and responded to sensitively, by those who love you more than anyone else, has far-reaching effects on long-term emotional security and health.
The Unicef UK Baby Friendly Initiative programme has been universal in changing attitudes and encouraging best practice over the last 20 years in the UK through robust accreditation. It delivers the minimum basic standards required to support new parents – no matter how they feed their babies. It aims to create the best environment for the start of every baby’s life but is not yet mandatory for all maternity facilities in England and Wales (see WBTi UK 2016 report – Part 1, Indicator 2).
The question is why isn’t it mandatory as recommended by NICE (the National Institute for Health and Care Excellence) 11 years ago? The guidance states: “All maternity care providers (whether working in hospital or in primary care) should implement an externally evaluated, structured programme that encourages breastfeeding, using the Baby Friendly Initiative as a minimum standard.”
The governments of Scotland and Northern Ireland have a funded national strategy with a coordinator supporting all maternal and infant health professionals, and 100% of maternity units in Scotland and Northern Ireland are accredited, with community facilities aiming to achieve the same.
This cascade of national to local support aims to ensure all parents receive the best possible information, free from the undermining effects of commercial persuasion, with practical support to be enabled to make healthy decisions for themselves, which helps fulfil the government’s health message.
Families would benefit if England and Wales followed the best practice example of their neighbours.
What does Baby Friendly care mean for parents? Relevant information from pregnancy onwards, skin-to-skin contact immediately after birth as standard practice, and practical help with learning how to feed your baby. For more details, see You can expect the following standards of care from aBaby Friendly hospital. If all expectant parents knew about the standards, they could help press for them to be implemented universally.
The WBTi UK report points out gaps and provides recommendations to overcome the many barriers that women face in their daily lives, journeying from pregnancy through birth, the postnatal months, back to work and beyond, living in their own communities. See Part 1, Indicator 2 of the report for more information, with further details in Part 2.
Implementing the WBTi recommendations would contribute to the provision of the optimal conditions all parents need to begin raising their child in a loving and supportive society.
The World Breastfeeding Trends Initiative (WBTi) is a tool to help countries assess their implementation of key policies and programmes. These are drawn from the WHO Global Strategy for Infant and Young Child Feeding, which was adopted by the World Health Assembly, including the UK. The first UK World Breastfeeding Trends Initiative report was published in November 2016 and launched at the Houses of Parliament. Its ten policy and practice indicators address the extent to which there is an infrastructure in a country to support breastfeeding. The process brought together organisations and agencies working in maternal and infant health to monitor progress, identify gaps and generate joint recommendations for action to address those gaps.
What is Indicator 1 about?
Indicator 1 asks if there is a national infant feeding policy, supported by a government programme, with a coordinating mechanism such as a national infant feeding committee and coordinator. The UK assessment found:
Women have autonomy over their own bodies so decide for themselves how to feed their babies but it can be very hard to carry a specific intention when the environment is unsupportive. It’s similar to the situation faced by someone who wants to avoid becoming overweight in an environment where tempting food is heavily advertised and easily available. A UK mother who wishes to breastfeed is likely to face barriers to achieving her goal throughout her breastfeeding journey.
National leadership
How can the situation be changed? An efficient way that can help to achieve consistency across the country is to have national leadership – a national coordinator with sufficient authority, a representative high level committee and a plan or strategy for change, as described in Indicator 1. Breastfeeding Policy Matters in 2015 highlighted the importance of this and the processes needed [1].
Scotland and Northern Ireland have national leadership in place but England does not. Yet the rhetoric is there. The 2016 government guidance from Public Health England, Health matters: giving every child the best start in life explains why the early years are so crucial [2]. It lists some of the health benefits and states that ‘creating the right environment to promote and support breastfeeding is crucial’. It highlights the importance of good maternal mental health so that the mother can be sensitive to the baby’s emotions and needs, helping the baby to develop secure attachment. Breastfeeding enhances a mother’s mental health while mothers who want to breastfeed but stop before they planned to are at greater risk of postnatal depression [3]. However, instead of increasing the support available to mothers, many support services were cut in 2016 because of reduced funds available. Such preventative services were not seen as a priority.
Freedom to choose how to feed one’s baby is valued in the UK and some people are concerned that mothers might feel pressured to breastfeed if it is encouraged. Ironically, advertising of follow on formula milks that might persuade mothers to switch from breastfeeding seems to cause less concern. Yet thousands of mothers make the often upsetting decision to stop breastfeeding before they wanted to. Where is the focus on these mothers and their suffering? Supporting breastfeeding is not about persuasion but about providing the infrastructure to enable them to continue; since some three quarters of mothers already opt to start breastfeeding, persuasion is irrelevant for them. If more mothers continued as long as they wished to, the proportion starting may well increase as expectant mothers will be less likely to hear negative messages.
Unicef UK’s widely endorsed Call to Action in 2016 included developing a national infant feeding strategy board in each nation [4]. What would a strategic plan encompass? The other WBTi indicators offer key points to include, such as Baby Friendly status being a universal goal, legislation in line with World Health Assembly recommendations, adequate protection for breastfeeding in the workplace, local support that is of high quality and integrated, and health professionals who have adequate training is supporting breastfeeding. If representatives of the four UK nations meet regularly they can also share ideas. Back in 2003 the World Health Organisation produced the Global Strategy for Infant and Young Child Feeding, which includes recommendations for national leadership, and this was followed in 2008 by the European Blueprint document [5,6]. Thus there are plenty of ideas available for developing a plan. The challenge is then implementation.
Alongside national leadership by governments, as described above, the breastfeeding support charities, relevant royal colleges and other similar professional bodies, campaigning organisations and interested individuals can both amplify calls for change and help to bring it about by collaborating. The infant feeding coalition meeting in June 2016, reinvigorating the idea of the former Breastfeeding Manifesto Coalition, demonstrated the keenness there is to work together [7]. Unicef UK’s Baby Friendly consultation on developing an inclusive Foundation provides an urgent opportunity to influence this – urgent because the deadline is 31 January 2017 [8].
Please read the consultation document and respond to the survey, thus helping to influence the future.
Also, check out our campaigning guidance for you to contact your MP and discuss issues highlighted in our report [9].
A baby is born and placed on his mother’s chest. His newborn reflexes kick in and he starts to crawl to her breast, calm and alert. This skin-to-skin contact triggers a surge in oxytocin – the so-called “mothering hormone” – and she responds by instinctively helping him to the breast. He latches on, and her milk flows.
When breastfeeding begins in this uninterrupted way, soon after birth, research shows that babies are more likely to breastfeed well, and mothers tend to continue to breastfeeding for longer.
Now compare this to the typical birth scenario, repeated in so many maternity hospitals:
A baby is born, and her cord is cut. The midwife announces “It’s a girl!” and then wipes the baby clean and wraps her up. Then she passes her to her mother. Then the baby is passed to her father. After a few minutes, the midwife unwraps the screaming baby and puts her on the scales and gives her a vitamin K injection. The baby is dressed and returned to her mother.
There is clear evidence for better outcomes for babies born in Baby Friendly hospitals – for example, a study in Scotland found that these babies are 28 percent more likely to be exclusively breastfed at 7 days old.
The meaning of Baby Friendly has also evolved over time, and in recent years it has moved beyond the ten steps. In the UK, as well as protecting breastfeeding, the Baby Friendly approach now helps mothers to begin a nurturing relationship with their baby – and this protection applies to all babies, whether or not they are breastfed.
The Baby Friendly Initiative has also moved beyond maternity hospitals. In the UK, it is now possible for university courses, health visitors, children’s centres, and neonatal units to become Baby Friendly accredited.
The World Breastfeeding Trends initiative (WBTi) assessment scores each country out of 5 based on how many Baby Friendly hospitals it has. It needs have more than 89 percent of its hospitals and maternity units accredited to gain the top rating.
The assessment also looks at the quality of the Baby Friendly programme – how comprehensive the training is, whether it monitors hospitals adequately, whether mothers’ experiences are taken into account – for another possible score of 5.






























{kind=link}