Imagine if every mother was entitled to the paid maternity leave, breastfeeding breaks and flexible return to work options she needed to enable her to combine breastfeeding with earning an income.
Please join the Global Breastfeeding Collective at a webinar to celebrate World Breastfeeding Week. Maternity leave and workplace accommodations are critical features of environments that enable breastfeeding. Hear from mothers about their experiences combining work and breastfeeding, get new ideas from countries who have used evidence-based policies to make breastfeeding work, learn about updated maternity leave recommendations, and find resources to support advocacy.
The Global Breastfeeding Collective is a partnership of more than 20 prominent international agencies, including the World Health Organization and UNICEF, calling on donors, policymakers, philanthropists and civil society to increase investment in breastfeeding worldwide.
This week’s topic in the “Breastfeeding: Not on the Agenda” series of webinars is the importance of planning for the protection of infant and young child feeding in emergencies, right here in the UK.
Infants, young children, pregnant and breastfeeding women are among the most vulnerable in any emergency situation, but they are almost invisible in our national resilience planning.
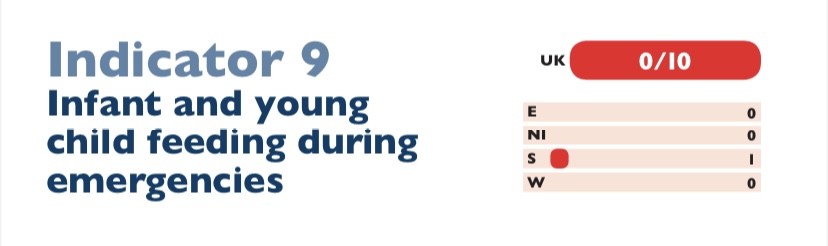
In the UK, the 2016 WBTi report found that while there is national guidance on the care of farm animals, pets, zoo animals and circus animals in emergencies, but there is no mention of infants or young children. There is an assumption that parents will take all responsibility for their own family – but too often there are no guidelines or recommendations to help them to prepare or handle an emergency.
Breastfeeding is a vital element in resilience and food security for families with infants: it provides immune protection and safe nutrition and fluids at any time, while providing both mother and child with comfort and resilience against stress. Skilled breastfeeding support is essential during emergencies, to enable breastfeeding dyads to continue.
In the UK, many infants are dependent on formula, which brings its own risks in an emergency. Infants who are not breastfed have reduced immunity to infections, in a situation where pathogens may be significantly increased due to contaminated water, or the crowding of evacuated families in rest centres. These infants depend on access to clean water, to a supply of suitable formula, and to hygienic preparation facilities and feeding equipment, and suitably trained support from responders and staff.
Local emergency planning in England and Wales is devolved to Local Resilience Forums (LRF). A recent study of LRF guidance for the public on emergency “grab bags,” by WBTi team member Patricia Wise, found that out of 42 LRF websites in England and Wales, only 27 even mention infant supplies, and 18 of those give only generic information rather than specific advice on what to pack for infants in an emergency. Northern Ireland included a generic ‘special equipment for children’ in its grab bag recommendations.
It is not difficult to include these supplies, facilities and training in every local resilience plan – there are resources and model operational guidance on the Infant Feeding in Emergencies Core Group website.
Contact your Local Resilience Forum (LRF) and ask them what they include in their “grab-bag” lists and their planning for rest centres in case of evacuation.
The climate crisis is contributing to increased frequency and severity of natural disasters. The Australian Government recently funded a large research project, Babies and Young Children in the Black Summer (BiBS) Study, into the impact of the Black Summer Bushfires on families with infants and young children, conducted by the Australian Breastfeeding Association, Dr Michelle Hamrosi and Dr Karleen Gribble from Western Sydney University. One of the findings from this study was that parents with young children felt that they did not have the right information in time, that they needed extra preparation and extra time to evacuate. In fact, the title of the BiBS report is “Want to help the children? Help the parents.”
The recent global COVID-19 emergency also had a disproportionate impact on families with infants and young children. Despite consistent guidance from WHO emphasising the importance of breastfeeding to infant health, and supporting mothers to maintain breastfeeding or at least their milk supply if possible, many countries routinely separated mothers and newborns, despite disrupting breastfeeding with the risks that would entail to maternal and infant health and wellbeing (Vu et al. 2020).
In the UK, families are also experiencing long term crises of food insecurity, especially during the current cost of living crisis. UNICEF Baby Friendly UK, NIFN and First Steps Nutrition have produced important guidance for local authorities on how to support these families. First Steps Nutrition have produced several related reports on food security for families with infants and on the impact of the cost of living crisis.
ACTION! contact your local authority and ask them
Whether they are implementing the UNICEF BFI guidance on food insecurity for families with infants
Whether your Local Resilience Forum plan includes infants and young children
Email us to tell us what you find out! wbti@ukbreastfeeding.org
Volunteer to help with WBTi’s research on infant feeding in emergencies for our upcoming second assessment of UK policies!
Ask your MP to ask questions about this in Parliament!
This webinar is part of the documentary and webinar series “Breastfeeding: Not on the Agenda” on breastfeeding, hosted by Dr Ernestine Ndzi from York St John University.
Previous webinars in the series and the documentary are available on YouTube.
Helen Gray is Joint Coordinator of the World Breastfeeding Trends Initiative (WBTi) project in the UK.
She is the Policy and Advocacy Lead for Lactation Consultants of Great Britain. She represents La Leche League of Great Britain on the UK Baby Feeding Law Group (BFLG), which works to bring the International Code of Marketing of Breastmilk Substitutes into UK law.
Helen’s background in anthropology and human evolution has influenced her interest in how breastfeeding, and the way we nurture our babies, are influenced by both human biology and culture.
Her current advocacy focus is the need for strong policies to protect infant feeding in emergencies. She has written several articles and chapters on the subject and served on the Advisory Panel for a London Food Resilience research project. She now represents BFLG on the global Infant Feeding in Emergencies Core Group.
August 1-7 will once again be World Breastfeeding Week. This year, the theme “Enabling Breastfeeding: Making a Difference for Working Parents” is all about combining working and breastfeeding.
One of the key findings from our first WBTi assessment of UK breastfeeding policies and programmes was that although the UK does provide paid maternity leave, and some paid paternity leave, and although there is some guidance on good practice from ACAS and from HSE, there is no statutory right in the UK to breastfeeding breaks or facilities in the workplace.
WABA produces regular snapshot Parents at Work reports on each country’s status on implementing International Labor Organization (ILO) conventions and recommendations on maternity protection at work, including maternity leave, paternity leave, and protected breaks for breastfeeding or expressing milk.
Breastfeeding-friendly workplaces provide time, income security and space to enable positive nutrition and health outcomes
All women should have the right to paid working time for breastfeeding, as called for by ILO Convention No. 183. In 2021, 138 countries provide a right to time and income security for breastfeeding. These provisions potentially benefit 8 in 10 potential mothers across the world. Since 2011, seven countries have introduced paid nursing breaks. However, breastfeeding breaks remain unpaid in four high-income countries. In 2021, at least four pathfinder countries recognize men’s supporting role by offering breastfeeding breaks to fathers.
Almost 5 in 10 potential mothers live in countries that grant two daily breastfeeding breaks; while 109 countries offer the right to daily nursing breaks for six months or more. This would support exclusive breastfeeding in line with World Health Organization (WHO) recommendations for 7 in 10 potential mothers across the world. However, only ten countries provide a right to breastfeeding breaks for at least two years, compromising mothers’ ability to continuing breastfeeding.
Workplace nursing facilities are a key ingredient of breastfeeding-friendly workplaces. However, only 42 countries offer the right to workplace nursing facilities, covering roughly 6 in 10 potential mothers globally. While small- and medium-sized enterprises (SMEs) are often exempted from these requirements, research shows that the economic and well-being benefits of breastfeeding for the new-born, the mother and the employer outweigh the limited costs of these measures. Only 13 countries offer a right to workplace nursing facilities irrespective of the number and sex of workers, with only 5 in 100 potential mothers worldwide living in these countries. Conditionalities for nursing facilities based on sex are discriminatory and remain in place in 19 countries.
WBW Action Folder
Details for campaigning for improved policies and support for breastfeeding in the workplace can be found in the World Breastfeeding Week Action Folder.
WBW Pledge Map
Organising a WBW2023 celebration? Add it to the pledge map!
Previous webinars in the series and the documentary are available on YouTube.
Thursday 3rd August at 1pm
‘Let’s make breastfeeding work – optimal maternity leave and workplace accommodations support an environment that enables breastfeeding’. Free webinar from the Global Breastfeeding Collective, led by WHO and UNICEF.
Maternity Action’s Senior Policy Officer Annah Psarros, on their new Toolkit for Employers, including a model Breastfeeding Policy
Saturday 5th August
Dr Ernestine Ndzi on Shared Parental Leave
Sunday 6th August
LCpl Natasha Day MBE, founder of the Defense Breastfeeding Network
Monday 7th August
Final blog from Dr Ernestine Ndzi on the need for “Family-Friendly Policies at Work”, and a Call to Action
Petition
And finally, everyone is encouraged to sign and share this petition from Dr. Ernestine Ndizi, calling for the government to:
Embed breastfeeding in the school curriculum and relevant health professional training.
Provide a policy on breastfeeding in the workplace which will protect the rights of breastfeeding mothers in the workplace.
Mandate all large public places like shopping malls, community centres, public libraries, museums, etc to provide breastfeeding rooms or spaces.
Fully adopt The Code of Marketing of Breastmilk Substitutes to protect babies and their families from harmful commercial influences and undermining of breastfeeding for commercial profit; and to protect families who formula feed from the escalating costs of premium brands.
Provide adequate 24/7 specialist lactation support in maternity services to actively counteract the culture of formula top-ups in hospitals; and to enable human donor milk to be more accessible as an option when mother’s milk is not immediately available.
Guarantee a sustained funding support to breastfeeding organisations who play a key part in supporting mothers.
– Include breastfeeding support on the Net Zero Environmental Agenda.
Do YOU want to be part of driving change for our children’s future?
The second assessment is now underway. It will run throughout this year and be launched in 2024.
What is the WBTi?
The World Breastfeeding Trends Initiative (WBTi) is a human rights-based, evidence-informed, collaborative and participatory national assessment of the implementation of key policies and programmes from the WHO’s Global Strategy for Infant and Young Child Feeding, and is a project developed by the International Baby Food Action Network (IBFAN). Currently nearly 100 countries are taking part.
WBTIIndicators of Policy and Programmes
National policy, programme, and coordination
Baby Friendly Initiative
International Code of Marketing of Breastmilk Substitutes
Maternity protection in the workplace
Health professional training
Community based support
Information support and communications
Infant feeding and HIV
Infant and young child feeding during emergencies
Monitoring and evaluation
In 2016, the UK scored just 50.5/ 100 on these ten key policy indicators.
WBTi brings together the main government agencies, health professional bodies, and civil society organisations involved in infant and maternal health and nutrition in each country to work together to collect information, identify gaps and generate recommendations for action. This Core Group must be free of conflicts of interest from the baby feeding industry (all infant or toddler milks up to 3 years, baby foods, bottles or teats).
The Global Breastfeeding Collective, led by WHO and UNICEF, recommend that the WBTi process be repeated, at least every 5 years, to monitor implementation of key policies, and include this in each country’s score on the Global Breastfeeding Scorecard.
Volunteers wanted
Many volunteers contributed to the success of the first UK WBTI assessment in 2016.
Your contribution is valuable, large or small:
Writing
Social media
Graphic design
Advocacy
Freedom of Information requests.
Fundraising
Mapping infant feeding training standards
Auditing numbers of breastfeeding counsellors and peer supporters
Project management
Virtual assistant skills
Parliamentary research
and more
You can find the main WBTi UK 2016 Report Part 1, and Part 2 with supplementary material, with Report Cards for each of the four nations and for the UK overall, here: https://ukbreastfeeding.org/wbtiuk2016/
WHO and UNICEF launched the Baby Friendly Initiative (BFHI) over thirty years ago; three years later, UNICEF UK Baby Friendly Initiative (BFI) was born. The original BFHI framework of Ten Steps was created to improve maternity and hospital practices that undermined breastfeeding, such as separating mothers and their newborns or routine formula supplements, as well as implementing the International Code of Breastmilk Substitutes in maternity settings, in order to eliminate conflicts of interest with the baby feeding industry (companies that manufacture or distribute infant formula/milks, baby foods, feeding bottles and teats) such as promotion of formula milk in healthcare settings, or direct contact by companies with parents.
The Baby Friendly Initiative has changed the face of maternity practices and midwifery training in the UK – breastfeeding initiation has gone up about 20% since UNICEF UK BFI was founded in 1994. In this country, BFI has grown beyond maternity settings to create standards for infant feeding support programmes in the community and for universities training the next generation of midwives and health visitors.The BFI standards were revised in 2012, based upon the twin pillars of breastfeeding and the UN Convention on the Rights of the Child.
Routine care: all staff in the universal services (midwives, health visitors, support workers etc) are trained to BFI standard with sound, evidence-based, basic training in supporting breastfeeding and responsive infant feeding.
Additional services: every area should have additional support available, such as trained, skilled peer supporters who can act as an “informed friend” for new mothers, and a network of local peer support groups where new parents can find social support alongside help with everyday breastfeeding issues.
Specialist services: every area should also have a referral pathway for specialist care for more complex breastfeeding problems; breastfeeding specialists should have extensive experience or training such as the IBCLC qualification or a recognised breastfeeding counsellor/supporter credential, and either be a registered health professional themselves, or co-lead the specialist service with a registered health professional.
WBTi poster on Integrated Services to Support Breastfeeding, 2019
A good example of how the BFI community standards work is Harrow. Read more HERE about how WBTi UK Steering Team member and specialist health visitor Alison Spiro led Harrow’s local community health services through BFI accreditation, to develop a well integrated services and become
“the only local authority in the UK where breastfeeding was the ‘normal’ way to feed babies”
More recently, UNICEF UK BFI have produced Learning Outcomes for a wider range of health professions: medical students, paediatricians, pharmacists, paediatric/ children’s nurses, maternity support workers and nursery nurses. These will help to address the gaps in high level health professional training standards found in WBTI’s 2016 report. Every health professional who works with women, infants and children should understand the basics of lactation and breastfeeding management, prescribing during lactation, and how to refer parents on to local breastfeeding support.
#WBW2022 Webinar
On Wednesday 3 August, we will all have the chance to learn more about the Ten Steps of BFHI in a webinar produced by the Global Breastfeeding Collective, an alliance of NGOs from around the world led by WHO and UNICEF.
In addition, there will be sessions on the care of young breastfed infants who are small or with faltering growth (the MAMI Pathway) and on infant feeding in emergencies.
The entire webinar runs from 7-9 AM BST and again from 4-6 PM BST, and will be recorded.
Skilled health professionals are a fundamental building block for successful breastfeeding. Parents expect all healthcare professionals to have the knowledge and skills to help them overcome practical challenges and to offer them emotional support. The reality in the UK is that many have not received the training they need to do this, so parents do not always receive the support they need. While improvements have been seen, UK health professional training still shows gaps in training in infant feeding. Relevant, evidence-based training is needed for all those who work with women, infants and young children.
WBTi findings: mapping UK high level health professional training standards in infant feeding against the WHO Educational Checklist
WBTi’s research has found numerous gaps in the pre-registration training in infant feeding in almost all UK health professional specialisms. Only midwifery training covers most of the topics on the WHO’s Educational Checklist on infant and young child feeding.
Alarmingly, the worst gaps are in the high level training standards for nurses, including paediatric nurses. Since the publication of our first report in 2016, there have been a few improvements in the training standards set for paediatricians and GPs, and our upcoming reassessment will be mapping these against the WHO checklist.
What can YOU do?
If you are a health professional,urge your governing body to strengthen the requirements on infant feeding in your professional standards and examinations by:
It takes a village to raise a child – we all have a role to play to support breastfeeding mothers and babies.
We all are the building blocks responsible for supporting new families: partners and family members, health workers, neighbours and community members, religious leaders, employers, academics, governments and policy makers. We can all make a difference. We need to step up to our responsibilities. Everyone needs to understand the importance of breastfeeding – for maternal and infant physical and mental health and wellbeing, for public health, for our economy, and for our planet.
For WBW this year, WABA has produced an extensive suite of materials looking at all these roles and responsibilities. They have outlined the challenges that breastfeeding families face at every stage from conception, through birth, getting breastfeeding off to a good start, and maintaining breastfeeding all the way through starting solids and going back to work, and the solutions we need in each situation – all backed up by links to the latest evidence.
The #WBW2022 Action Folder pulls all this together: it is a useful resource for anyone using evidence to build policies and best practice. You can download it as a PDF and all the links to research and references will be live.
The UK WBTi team will be highlighting just a few of the concepts this week:
Health workers: the importance of relevant, evidence-based. The advertising of follow-on milks, on the media, from 6 months in the UK has led to confusion, resulting in some parents seeing formula milk as equivalent to breastmilk, or that breastfeeding should stop at 6 months. The International Code needs to be adopted by the UK government in full, to reduce this confusion and protect breastfeeding. training for all those who work with women, infants and young children
UNICEF UK Baby Friendly Initiative and the BFHI worldwide sets out ways in which healthcare staff can receive sound, evidence-based, basic training in supporting breastfeeding.
ALSO join a special webinar from the Global Breastfeeding Collective on BFHI, with some added specialist topics on supporting small and underweight breastfeeding infants, and on infant feeding in emergencies. (7-9 AM BST and again at 4-6 PM BST). Register HERE
Community support: Access to skilled, integrated support for all, with a special focus in the GBC webinar on how to support breastfeeding infants who are not gaining well (NICE NG 75,2017). All parents should have easy access to trained healthcare staff- midwives, paediatricians, health visitors and GPs- breastfeeding peer supporters and specialist support (IBCLC, BFCs). Supporting breastfeeding in complex circumstances: Specialist support from IBCLCS, BFCs, or infant feeding leads, integrated with specialist healthcare teams
Protecting infants and young children in emergencies. National policies should guide Local Resilience Forums but these do not exist at present.
The impact of misleading marketing: The International Code. The advertising of follow-on milks, on the media, from 6 months in the UK has led to confusion, resulting in some parents seeing formula milk as equivalent to breastmilk, or that breastfeeding should stop at 6 months. The International Code needs to be adopted by the UK government in full, to reduce this confusion and protect breastfeeding.
Governments with national and local policy makers need to protect all families and support them to make informed feeding decisions free of commercial influence.
What can YOU do?
It is time for a reassessment of the UK’s national infant feeding policies and programmes. YOU could help! Volunteers are welcome with knowledge in any of the ten policy areas (Indicators 1-10), or with skills such as research, writing, graphics, social media and more – feel free to contact us for a chat!
WBTi Key Indicators:
Indicator 1: National policy, programme and coordination Indicator 2: Baby Friendly Initiative Indicator 3: International Code of Marketing of Breastmilk Substitutes
Indicator 4: Maternity protection Indicator 5: Health professional training Indicator 6: Community-based support Indicator 7: Information support Indicator 8: Infant feeding and HIV
Indicator 9: Infant and young child feeding during emergencies
Indicator 10: Monitoring and evaluation
Which one will YOU choose?
Contact us: wbti@ukbreastfeeding.org
Helen Gray MPhil IBCLC is Joint Coordinator of the WBTi UK Steering Group.
The Week runs from June 27th to July 2nd and the theme is ‘Everyone has a part to play in helping mums to breastfeed’. The early weeks with a new baby are hard for most mothers and some find that time very challenging but support can make a huge difference. Some people around the mother, particularly partners, can offer practical help in looking after the home and the mother so that she can recuperate after the birth and focus on nurturing the baby, which primarily means feeding.
Sometimes skilled support is needed to enable breastfeeding to work better, which often means improving the latch. This can be from health professionals, such as midwives and health visitors, and specialists – breastfeeding counsellors and IBCLCs (International Board-Certified Lactation Consultants); the specialist services include national helplines*. Trained breastfeeding peer supporters are available in many areas and can offer invaluable mother-to-mother support. They often work in volunteer or paid roles in local support groups, where mothers can give each other confidence and build self-reliance through sharing their stories.
Everyone having contact with the mother can be emotionally supportive, indicating that they value what she is doing and respect her decisions, helping to build her confidence that she can make breastfeeding work. These includes friends, relatives, neighbours, GPs, pharmacists, shop staff…
However, alongside these personal contacts, society’s infrastructure and attitudes can also influence a mother’s experiences with infant feeding. A World Breastfeeding Trends Initiative assessment demonstrates the extent to which a country’s support for breastfeeding implements the Global Strategy on Infant and Young Child Feeding, by scoring ten policy and programme indicators:
1. National policy and funding
2. Baby Friendly in maternity settings
3. WHO International Code of Marketing of Breastmilk Substitutes (the Code)
4. Maternity protection in workplaces
5. Health professional training
6. Support services for pregnant and breastfeeding mothers
7. Accurate and unbiased information
8. Infant feeding and HIV
9. Infant and young child feeding during emergencies
10.Data – monitoring and evaluation
The UK assessment in 2016 showed the variability between indicators, particularly as an assessment identifies gaps and makes recommendations.
2016 UK report
Carrying out a WBTi assessment in a country around every 5 years monitors the progress, or lack of it, in a country. It is time for a reassessment in the UK.
If you would like to be involved in collecting data, please do contact us, and let us know which of the indicators above YOU are interested in?
Our WBTi work has revealed that in the UK we have no national guidance on the support and feeding of infants and young children, or pregnant or breastfeeding mothers, during emergencies. There is currently a postcode lottery of Local Resilience Forums who include a few details in their advice to the public such as “Remember to pack formula and nappies for your baby”, but there is no national guidance for LRFs and local authorities that they should include infants and young children in their planning.
This page will serve as a repository for resources for those planning services and those providing feeding support for Ukrainian families with infants and young children.
Breastfeeding provides infants with food security, immune protection, and emotional comfort during disasters. Basic priorities in an emergency:
1) Support new mothers to hold their babies skin to skin and begin breastfeeding within the first hour.
2) Support mothers who are breastfeeding, partially or fully breastfeeding, to continue breastfeeding and increase their milk supply if needed: provide access to skilled feeding support.
3) Protect infants who are not breastfed: Trained infant feeding / nutrition support teams from trusted NGOs like UNICEF will provide access to safe supplies of appropriate infant formula for babies that need it, and support with safe preparation under hazardous conditions.
4) Protect all infants: breastmilk substitutes and feeding equipment (infant formulas and other milks, bottles, teats, breast pumps and also donor human milk) will be provided by trusted NGOs like UNICEF; the public should AVOID sending donations of these into high risk settings, but send donations of funds to trusted NGOS instead. This will enable them to provide families with what is needed on the ground.
These organisations are members of the Infant Feeding in Emergencies Core Group and have created the international Operational Guidance on Infant Feeding in Emergencies. Please consider supporting their work with families with infants and young children.
We have collected links to infant feeding resources in Ukrainian, and also in the languages of countries housing refugee families, for breastfeeding helpers and aid workers in those countries.
Please send us any suggestions for additional resources
We have a few other resources not included here; please email us any enquiries.
NOTE: we will continue to add links and resources to this page, and these organisations are continuing to add further translations into more languages – please make sure that you clear your cache, or ‘refresh’ the page, each time you open any of these links to ensure that you find the most up to date page.
NOTE: We are providing these resources as a public service, but we cannot read the resources in other languages ourselves, so we cannot always vouch for the accuracy of the contents. Please have someone fluent in the language read it for you.
Guidance for helpers not trained in supporting infant feeding
This short leaflet was written for local authorities and those supporting Afghan refugee families but could be useful for those supporting Ukrainian refugees in the UK. It sets the context, lists some useful resources for parents, provides information about making up powdered infant formula correctly and describes useful actions in some possible scenarios.
Infant feeding support resources – multiple languages
Pictorial counselling cards in many languages including Russian, adapted to include COVID19 recommendations. Some are full pictorial sets, while some are simply the translation matrix.
Infant Feeding flyer for families in transit (including English, Ukrainian, Polish, Russian, updated for COVID19). Developed by the volunteer team from Infant Feeding Support for Refugee Children/ Safely Fed
Pictorial book about breastfeeding (no words) from La Leche League Netherlands. The PDF is free to use for all. Printing and sharing is allowed, as long as the original file (including credits) is unaltered. Price listed on website is for printed version.
Breastfeeding Matters – A Guide to Breastfeeding for Women and their Families (from best Start, Ontario Canada) can be downloaded free in Russian and other languages
La Leche League International: Variety of resources and infographics in infant feeding in emergencies translated into multiple languages – most are directed at mothers and parents
Please do contact us if you are interested in volunteering or have some useful resources to share!!
CONTACT: wbti@ukbreastfeeding.org
Helen Gray MPhil IBCLC is Joint Coordinator of the WBTI UK Steering Team, and Policy and Advocacy Lead at Lactation Consultants of Great Britain. Her research interests include human rights and infant and young child feeding in emergencies.
A shocking new report on formula marketing which was commissioned by the World Health Organisation and Unicef has been launched. Called ‘How the marketing of formula milk influences our discussions on infant feeding’, it is a large scale and thorough report in which women’s voices are a key part. The report can be downloaded from this page.
Eight countries were included (Mexico, Bangladesh, UK, Vietnam, S. Africa, Nigeria, China and Morocco) and it involved 8500 mothers talking about their experiences of being targeted and also interviews with health professionals and marketing executives. The survey was conducted by M&C Saatchi World Services, which states on its website: “Our aim is to harness the power of cutting-edge marketing, communications and creativity, so that they become key tenets of behaviour change activity throughout the International Development sector.”
The conclusions of the report are that the marketing is highly targeted, pervasive and exploitative, uses misleading scientific claims and incorporates appeals to aspiration. It therefore backs up robustly what has been known about infant formula marketing for many years. Industry invests more in marketing each year than the funds WHO has available!
‘Marketing the $55 billion formula milk industry’, the webinar of the launch of the report on 23 February is available here.
What needs to happen:
1. Invest in mothers and families (e.g. good maternity legislation)
2. Protect the integrity of science and medicine (including strong conflict of interest policies)
3. Urgently legislate, regulate and enforce regulations in order to protect all families.
The launch was hosted by Kathriona Devereux, science communicator and Cuidhu breastfeeding counsellor, on behalf of WHO, Unicef, Save the Children and two other organisations. Dr. Nigel Rollins gave a brief history of infant formula marketing and presented the key findings. Anu Narayan of Unicef framed the issue – it’s about marketing, the right to accurate and impartial information, and public health v commercial interests, not about breastfeeding v bottle feeding or limiting access or rights. The study questions were:
What are women’s experiences of and attitudes towards formula marketing?
What are health professionals’ experiences of and attitudes towards formula marketing?
The presentation was followed by comments from a panel that comprised Helen Clark (former Prime Minister of New Zealand), Rebone Ntsie, dietitian from South Africa, Duong Vu from Alive and Thrive in Vietnam, Professor Caroline Homer, specialist in maternal and infant nutrition, and Katie Gilbert, Managing Director at M&C Saatchi World Services. Recommendations for action from the panel included: framing the issues as supporting the right to health, engaging political leaders, recognising the scale and urgency of the problem, improving national regulations and checking imports comply with regulations. It was also suggested that public health needs both to provide the services that mothers need and to demonstrate empathy in its communications, as breastfeeding counsellors are trained to do, indicating understanding of what it’s like to be a mother; formula marketing conveys that impression of understanding.
Worryingly, updating the International Code to address marketing through social media better was also suggested; however, the Code has been updated by 19 subsequent resolutions since 1981 to close loopholes and it does cover all marketing. Governments need to have strong enforceable regulations to implement the Code and resolutions, including addressing digital marketing, and thus protect infants and young children.
What wasn’t mentioned was the significant negative environmental impact of formula feeding. Protecting and supporting families who want to breastfeed to do so will reduce that negative impact.
In addition there is a petition to stop unethical formula research on babies, and particularly a new study in Africa in which low birthweight exclusively breastfed babies will randomly be allocated formula.
If you’d like to check the content of the current UK Laws, the Baby Feeding Law Group (BFLG) has information and links on its website.
Author
Patricia Wise is an NCT Breastfeeding Counsellor and a member of the WBTi UK Steering Group