The year 2020 has seen us facing unprecedented multiple crises and emergencies:
· COVID19
· The Climate Emergency
· A crisis propelling equity, racial and social justice to the forefront through #BlackLivesMatter
The global theme of World Breastfeeding Week 2020, “Support breastfeeding for a healthier planet,” is a focus on the Climate Emergency, and the impact of infant feeding on our environment and the planet.
#SupportBreastfeedingforaHealthierPlanet
We can all think of so many ways that breastfeeding is good for the planet – no food miles at all, no pollution or litter from manufacturing or distribution, a very small carbon footprint to feed a breastfeeding mother rather than a herd of cows! Most mothers in the UK want to breastfeed, and mothers are already doing the best they can. It is really our governments and policy makers who need to wake up to this, and they who should provide the policies and programmes that families need to breastfeed. And it is our governments who have the responsibility to plan a “green recovery” from COVID19, so that we can return to a healthier world for everyone.
“Overall, breastfeeding for six months saves an estimated 95-153kg of CO2 equivalent per baby”. This comes from an 2019 BMJ editorial by Joffe, Webster and Shenker called Support for Breastfeeding is an environmental imperative. Yet only 1% of babies in the UK are exclusively breastfed for six months (PHE).
Most formula is based on cows’ milk, and dairy farming has a significant burden of greenhouse gases, both carbon and methane. (GreenFeeding). Processed, powdered formula milk has a large water footprint as well – up to 4700 litres for every kg of milk powder! (IBFAN)
Bottle feeding also requires multiple plastic bottles and teats, as well as fuel to boil water, sterilise equipment, and store formula safely. Bottle feeding in hospitals creates waste, as described by Becker and Ryan-Fogarty in the BMJ.
One example of a government policy that could support families and reduce the need for these would be breastfeeding breaks at work, and childcare close by. This would enable mothers to feed their children themselves, without the additional burden of expressing and storing their milk. Going back to work was cited as one of the main reasons that women stopped breastfeeding early.
There will always be a need for formula and bottles for those babies who cannot be breastfed. But most mothers in the UK do want to breastfeed, and it is the responsibility of our government, of our health system, and our local authorities, to provide the policies and programmes to enable women to continue breastfeeding as long as they want to.
With breastfeeding support under strain, service providers propose plan to tackle inequalities
This World Breastfeeding Week (1-7 August 2020), #WBW2020 and #GreenFeeding, we are calling on the UK government to address the fragility of breastfeeding support services.
Our organisations have seen first-hand how the Covid-19 crisis has exposed the fragility of infant feeding support available for women, parents and families.
Over the past few months, the need to support babies and families has escalated and support services have been stretched beyond anything in our experience.
Existing variations in provision for infant feeding support have increased as services have been cut, health visiting teams redeployed and provision moved online, leading to unknown outcomes on infant nutritional health, worsening maternal mental health and widening health inequalities.
Tremendous efforts from the NHS and Third Sector organisations, including many volunteers on the National Breastfeeding Helpline and other charity-run helplines, along with swift adaptation to offer online support, have provided many families with support but this is not sustainable without a longer term strategy.
Meanwhile, the need to protect infant and young child feeding in pandemic emergencies has not previously been considered and has been entirely missing from the Scientific Advisory Group for Emergencies’ reports.
Investing in the health of new families, including supporting and protecting breastfeeding and supporting safe and responsive formula or mixed feeding, enables children not just to survive, but to thrive.
Rebuilding infant feeding support for communities after Covid-19 and giving important attention to the needs of mothers and children from Black, Asian and minority ethnic backgrounds will help tackle inequalities.
Infant feeding is a critical component of first 1001 Days and Early Years Health
We welcome the appointment of Andrea Leadsom MP as the Government’s Early Years Health Adviser and the announcement of a review at a time when infant feeding support services for women, parents and families have been stretched to an unprecedented degree.
Protecting breastfeeding and ensuring safe and responsive formula and mixed feeding during those first 1001 days would make a significant contribution to reducing inequalities in health. As a result, it also upholds the work of the NHS and helps build a healthier population.
While COVID-19 has undoubtedly placed a strain on support systems, it has also highlighted a huge omission in UK policy on planning for the care and feeding of infants and young children in case of emergencies, leaving our youngest members of society vulnerable.
While the benefits of breastfeeding are well-evidenced, merely stating these benefits does not ensure breastfeeding is protected or supported. At a time of global health crisis, and increasing recognition of the impact of human behaviour on the health of our planet, support for breastfeeding is also an environmental imperative.
10-point Infant Feeding Action Plan to address Inequalities
We call on the UK government to adopt the following 10-point Infant Feeding Action Plan below which has a particular focus on working to reduce inequalities:
For the new Government Early Years Advisor to appoint a permanent, multi-sectoral maternal, infant and young child nutrition strategy group to implement a national strategy to support good nutrition across the first 1001 days.
To commission and sustainably fund universal, accessible, confidential breastfeeding support delivered by specialist/lead midwives, health visitors and suitably qualified breastfeeding specialists, recognising the role of charitable organisations and community groups and their strong links with communities.
To ensure there are children’s centresor family hubs, disproportionately located in areas of disadvantage, offering joined-up universal services that include breastfeeding peer support, guidance on the introduction of solids and eating well in the early years.
To ensure that health visiting services are properly funded and the number of health visitors increased to ensure consistent timely nutritional support for all families to support good maternal and infant mental and physical health.
To integrate planning to support infant and young child feeding in emergencies into legislation, the Civil Contingencies Act, and Local Resilience Forums across the country.
To recognise the importance of breastmilk for preterm and vulnerable babies and the need for equitable access to donor breastmilk for these babies through the establishment of a fully funded regional donor milk banking service.
To implement the Unicef UK Baby Friendly Initiative across community, hospital and neonatal services, building on the recommendation for all maternity services to be accredited in the NHS Long Term Plan.
To make it a statutory right of working mothers to access a private space and paid breaks to breastfeed and/or express breastmilk and manage its safe storage.
To support the commitment to re-instate the quintennial Infant Feeding Survey which builds on data previously collected every five years since 1975, most recently in 2010.
To protect babies from harmful commercial interests by bringing, as a minimum, the full World Health Organisation International Code of Marketing of Breastmilk Substitutes into UK law and enforcing this law.
The Breastfeeding Network Association of Breastfeeding Mothers NCT La Leche League GB HENRY Institute of Health Visiting Best Beginnings Human Milk Foundation Local Infant Feeding Information Board Lactation Consultants of Great Britain World Breastfeeding Trends Initiative UK Hospital Infant Feeding Network GP Infant Feeding Network UK Association of Milk Banking Diversity in Infant Feeding Better Breastfeeding Nursing Matters Save Time Support Breastfeeding Swansea University Breastfeeding Twins and Triplets
The year 2020 has seen us facing unprecedented multiple crises and emergencies:
COVID19
The Climate Emergency
A crisis propelling equity, racial and social justice to the forefront through #BlackLivesMatter
The global theme of World Breastfeeding Week 2020, #WBW2020 and #GreenFeeding, “Support breastfeeding for a healthier planet,” is a focus on the Climate Emergency, and the impact of infant feeding on our environment and the planet.
When the novel coronavirus hit it reminded us that we are all linked, one people on one planet.
Breastfeeding and COVID-19
Some of those people were breastfeeding mothers and babies. At first, medical protocols for isolating COVID+ patients dictated that some mothers and babies were separated. Slowly the evidence accumulated that breastmilk itself did not appear to transmit the virus, and in fact antibodies to COVID19 began to be found in mothers’ milk. Now there are even research projects investigating whether the antibodies to COVID-19 in breastmilk could be used to protect others!
In the UK, the Royal Colleges who work with mothers and babies, led by the Royal College of Obstetricians and Gynaecologists (RCOG) and the Royal College of Midwives (RCM) quickly began to produce joint guidance, updated weekly. This was hosted on the RCOG website and became a global point of reference.
Coronavirus (COVID19) infection and pregnancy: this clinical guidance contains their influential recommendations on keeping mothers and babies together in hospital after birth, whether or not the mother is COVID+, and their recommendation that staff support the mother to breastfeed or express her milk for her baby, unless the mother is too ill. These recommendations have influenced health policy around the world, keeping many mothers and babies together worldwide.
A useful Q&A page of information for women and their families, written in plain language.
Guidance for antenatal and postnatal services during the evolving coronavirus (COVID19) pandemic. This includes some information on the management of breastfeeding in the community, including the following : “Remote support by third-sector organisations will be invaluable to provide support for breastfeeding, mental health and early parenting advice.”
The World Health Organisation has produced a steady stream of updates and resources emphasising the importance of breastfeeding during the COVID crisis. This includes:
a media briefing on the 12 June at which the Director-General stated:
“WHO has also carefully investigated the risks of women transmitting COVID-19 to their babies during breastfeeding.
We know that children are at relatively low-risk of COVID-19, but are at high risk of numerous other diseases and conditions that breastfeeding prevents.
Based on the available evidence, WHO’s advice is that the benefits of breastfeeding outweigh any potential risks of transmission of COVID-19.
Mothers with suspected or confirmed COVID-19 should be encouraged to initiate and continue breastfeeding and not be separated from their infants, unless the mother is too unwell.
WHO has detailed information in our clinical guidance about how to breastfeed safely.”
We recommend that mothers with suspected or confirmed COVID-19 should be encouraged to initiate and continue breastfeeding. From the available evidence, mothers should be counselled that the benefits of breast-feeding substantially outweigh the potential risks of transmission.
In the UK, breastfeeding services suffered as midwifery and health visiting staffing levels were reduced by illness and self isolation, some staff were redeployed to labour ward or public health, childrens’ centres and breastfeeding support groups were closed. Families were discharged with their new baby to go home to a changed world, isolated in their home. Most health professional contacts were now virtual, and there were few opportunities to have baby weighed or seen in person, so parents were left on their own to figure out if their baby was doing well.
In areas like Brighton, with a strong, integrated commissioned NHS breastfeeding support programme, with a well embedded, large trained peer support programme and where there is a specialist NHS IBCLC clinic for complex problems, all the NHS support simply moved online. Once the technical side of this was worked out, breastfeeding support was still there for those who needed it.
In other areas, that depended on health visitors alone to deliver all the breastfeeding support, where there was no peer support commissioned and no specialist clinic staff, once the childrens’ centres were closed and many health visitors redeployed to other public health roles during the COVID-19 crisis, there might be one infant feeding lead health visitor left in the whole community.
Across the country, breastfeeding organisations and breastfeeding supporters sprang into action. Calls to the National Breastfeeding Helpline rose significantly, and trained volunteers turned out in droves. NCT moved their antenatal classes online, La Leche League local groups and NCT breastfeeding support groups moved onto Zoom, and IBCLCs set up remote consultations. A new app was trialled through the NHSX TechForce19 competition, Peppy Baby, in collaboration with Lactation Consultants of Great Britain and NCT, providing free access to online support groups and even video consultations for specialist breastfeeding help and mental health support. Suddenly there was online breastfeeding support available somewhere, every day of the week.
This had some advantages: mothers could join a Zoom meeting with their baby, still in bed. No one had to travel to get help. But some families had complex situations that did need face to face support, and it could be a challenge to find a specialist who could provide face to face support, or a tongue tie clinic that was still open.
Some families were able “nest” in isolation, with both parents home and no visitors, and flourished. Others struggled without face to face contact, without weight checks for baby, or struggled with their mental health. It will be hard to unpick the outcomes, as in many areas the usual health visitor checks were no longer taking place in person, so there are many gaps in the data. For instance, in some areas, no-one collected breastfeeding rates at 6-8 weeks, so it will be difficult to see the impact of COVID-19 on breastfeeding there.
It is vital that we all call on our local authorities, our CCGs and our Local Maternity Systems to rebuild a stronger network of skilled breastfeeding support as we come out of this first COVID-19 crisis – we must be more prepared for the next one.
This is the start of World Breastfeeding Week 2020, which runs from the 1st to the 7th August. WBW is a global campaign to raise awareness and galvanise action on themes related to breastfeeding and commemorates the 1990 Innocenti Declaration. Since 2016, WBW has been aligned with the United Nations’ Sustainable Development Goals.
Breastfeeding can be hard in the early weeks under normal circumstances, adjusting to meeting the needs of a vulnerable human being, including urgent frequent feeding, and the tiredness that results from being on call 24 hours a day, 7 days a week. If feeding is painful it feels even harder. That is why having skilled breastfeeding support readily available, for any mother that needs it, is so important. Breastfeeding usually becomes much easier and more enjoyable as the weeks pass, especially if worries about painful feeds or milk supply or difficulties due to causes like tongue-tie are resolved, and is helped by babies tending to have more spaced and shorter feeds.
This year Covid-19 lockdown has been an added complication, particularly for new families as they have minimal face-to-face contacts.
What have the challenges and highlights been for you? You can share your experiences using the Leave a Reply box below.
A new study by trainee doctor Kirsty Biggs and senior colleagues has shown that 97% of the 411 medical students who responded to a survey are uncertain of their practical skills to support new mothers with breastfeeding, such as helping with latch issues, although the overall benefits of breastfeeding were moderately well-known. Yet most students (93%) perceived doctors to have an important role in supporting breastfeeding and the same percentage requested further breastfeeding education.
Over 80% of the respondents had a career interest in obstetric and gynaecology, paediatrics and/or general. While the sample was only around 1% of UK medical students, and only one-quarter of the students responding were male, it’s a very clear message that breastfeeding education overall is not adequate.
Around 80% of the 32 UK medical schools eligible responded to their part of the survey and results indicate that only 70% of medical schools provide compulsory breastfeeding education.
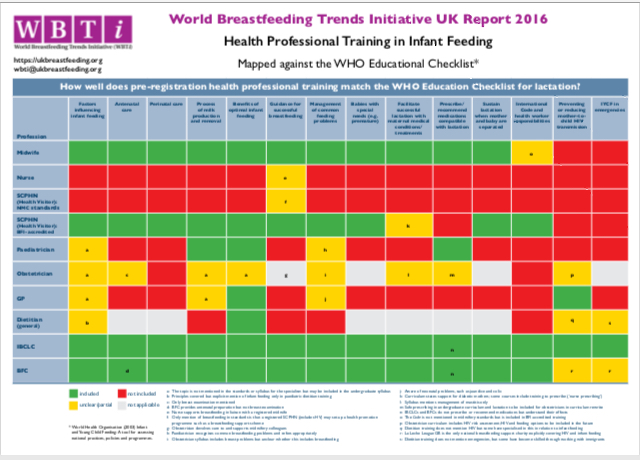
WBTI’s findings and vision
The WBTi UK report in 2016 indicated that medical curricula have many gaps with regard to breastfeeding, and Biggs’ study confirms that the students themselves find it inadequate. WBTi UK’s vision is that all doctors have sufficient training in infant feeding to protect the decisions of mothers who want to breastfeed.
How can the situation be improved? High level standards and Unicef BFI learning outcomes
The General Medical Council provides broad guidelines for undergraduate curricula in its Outcomes for Graduates document and each medical school devises its own curriculum to fit the guidelines. For example, the expectation under the Outcomes Health promotion and illness prevention section is: ‘Newly qualified doctors must be able to apply the principles, methods and knowledge of population health and the improvement of health and sustainable healthcare to medical practice’. Unicef UK Baby Friendly Initiative’s learning outcomes for several professions, including medical students, published in November 2019 are highly relevant to improving curricula and accompanying resources are being developed.
RCPCH curriculum – an encouraging sign
Medical training is long, with undergraduate, Foundation and then specialty training. The RCPCH (Royal College of Paediatrics and Child Health) states as part of its activity to promote breastfeeding: ‘The RCPCH training curriculum for General Paediatricians and all paediatric subspecialties requires training to understand the importance of breastfeeding and lactation physiology, be able to recognise common breastfeeding problems, have knowledge of formula and complementary feeding, and be able to advise mothers or refer for support.’
Mentioning infant feeding in guidance to doctors to encourage including it in consultations is also important. GP Louise Santhanam (founder of GPIFN) is the lead author of Postnatal Maternal and Infant careduring the COVID-19 Pandemic: a Guide for General Practicethat was recently added to the RCGP website. This clarifies that 6-8 week checks need to continue despite the Covid-19 pandemic and that infant feeding should be a routine clinical consideration.
Thus plenty of resources are available but doctors are busy people. While some really understand the importance of protecting breastfeeding, and know how to – such as signposting mothers to local skilled help – the challenge is how to bring this into every medical student’s training.
If you know anyone at medical school, it would be really useful if you can let them know about Kirsty Biggs’ study.
This week (7- 12 June) is Infant Mental Health Awareness Week and the theme is ‘20:20 vision: Seeing the world through babies’ eyes’. The Week is led by the Parent-Infant Foundation (PIF) and theFirst 1001 Days Movement, a collaboration of relevant organisations with the PIF as secretariat, which is being launched during the week.
What is infant mental health? It is the emotional wellbeing of babies. The Movement’s vision is that ‘every baby has loving and nurturing relationships in a society that values emotional wellbeing and development in the first 1001 days, from pregnancy, as the critical foundation for a healthy and fulfilling life.’
What babies want is what they need and these needs are basic. As obstetrician Grantly Dick-Read wrote in the mid 20th century:
“The newborn has only three demands. They are warmth in the arms of its mother, food from her breasts, and security in the knowledge of her presence. Breastfeeding satisfies all three.”
They do also need to receive attention from other humans. If their needs are usually met, babies can form secure relationships (attachment) with their caregivers. Usually, there is one primary caregiver, most commonly the mother. Attachment theory was developed by the psychoanalyst John Bowlby in the 1950s. An attachment figure who cares responsively for the infant provides a secure base. It is believed that behaviours by the infant to stay close when separated, like screaming and clinging, have been reinforced by natural selection (see What is attachment theory).
Babies are vulnerable – as Donald Winnicott, paediatrician and psychoanalyst, among his other insightful quotes, stated:
‘There is no such thing as a baby, there is a baby and someone’.
However, infants are not passive as they communicate by giving cues to their needs, such as the rooting reflex when hungry. If their needs are not responded to quickly, they become upset. Dr. Edward Tronick’s ‘still face’ experiments in the 1970s showed the importance of human connection for an infant. If the parent’s face is still and unresponsive to her baby, the baby looks confused and then becomes distressed. The experiments also showed that ruptures in a relationship like this are easily repaired. Parents do not need to respond perfectly.
However, when there is repeatedly no response to a baby’s distress, as in sleep training where the baby is left alone and expected to adapt, it was found that the babies’ behaviour changed so that by the third night they were no longer crying but their cortisol (stress hormone) levels were still high so there was a mismatch between behaviour and physiology; instead of learning to self-soothe it seems as though they were giving up so in despair.
The significance of the care babies receive is that their experiences, starting before birth, influence the neural connections that are formed in the developing brain – the ‘wiring’. A parent who is emotionally not really available to the baby (so not attuned to their needs) will find it difficult either to respond or to respond appropriately, providing an unintentional ‘still face’ or angry face. The parents could be ill, depressed, addicted, suffering domestic abuse, desperately worried about their financial situation, overloaded with responsibilities………It is therefore crucial for a society to care for parents so that they can be emotionally available to their children.
Feeding is a crucial part of nurturing care and breastfeeding facilitates the process.There is considerable evidence that not being breastfed is linked to poorer physical health in infants (Lancet, 2016). Breastfeeding provides personalised nutrition. Antibodies and other components in breastmilk reduce the chance and severity of infections. Oligosaccharides in breastmilk feed and thus favour beneficial bacteria in the infant’s gut and this helps the development of a healthy immune system. It is difficult to allow for confounding factors in studies on breastfeeding but reviews show it is linked with better cognitive performance, which is likely to be due to the fatty acids in breastmilk. But what about any impact on emotional development? There are studies which suggest that being breastfed is associated with paying more attention to positive emotions in others. Breastmilk contains the calming hormone oxytocin, which stimulates social interactions, and which is further released through touch and suckling, so the moods of both mother and baby benefit. Several studies indicate that mothers who are breastfeeding tend to touch their babies more, are more responsive and tend to gaze at them more, all of which will help the infant’s emotional wellbeing. The Unicef UK Baby Friendly Initiative leaflet, Building a Happy Baby, provides practical suggestions for parents to support their baby’s brain development and addresses myths and realities.
Mothers who stop breastfeeding before they want to are at greater risk of postnatal depression (Borra et al 2014) so mothers need easy access to breastfeeding support to help them continue, thereby benefitting their babies physically and emotionally. Sadly, there are barriers to breastfeeding throughout society, as outlined in the WBTi UK report.
Parents and carers urgently need more support, especially during the stresses and isolation of lockdown and the COVID19 pandemic. We call on government to make infants and their families a high priority during the pandemic and in our plans to rebuild a stronger society.
Photo used with permission
Patricia Wise is an NCT breastfeeding Counsellor and a member of the WBTi UK Steering Group
The Covid-19 pandemic has shown how important it is for countries to protect their citizens from illness.
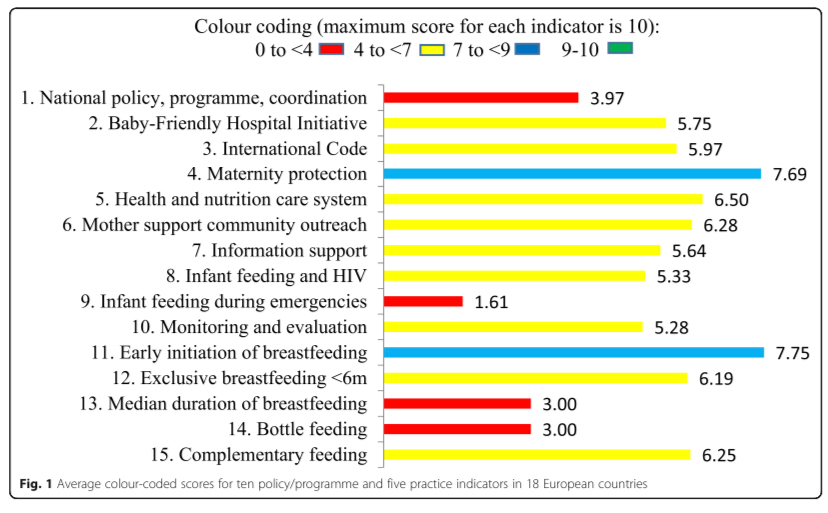
Yet a new WBTi regional report shows gaps in support for families across Europe, with the poorest overall scores in national leadership and, shockingly, emergency preparedness, where the UK scored 0/10. This pandemic is an emergency for infants and young children and only North Macedonia was found to have an adequate strategy.
Babies who are breastfed have better health and resistance to infection, and most mothers want to breastfeed. Yet many European mothers stop or reduce breastfeeding in the early weeks and months, and bottle feeding is prevalent, due to inadequate support from health systems and society.
Launched today, the first European report on infant and young child feeding policies and practices, Are our babies off to a healthy start?, compares 18 countries and identifies the considerable improvements they need to make in supporting mothers who want to breastfeed. A summary report has been published today in theInternational Breastfeeding Journal.
The new report, Are our babies off to a healthy start?, compares the implementation of WHO’s Global Strategy for Infant and Young Child Feeding across 18 European countries. The comparisons show clearly that inadequate support and protection for breastfeeding mothers is a Europe-wide problem. The health of babies, mothers and whole populations lose out as a result. However, countries do differ considerably. Turkey rates highest overall; the five countries with the lowest scores belong to the European Union.
‘Nutrition is key to achieving the Sustainable Development Goals related to health, education, sustainable development, reduction of inequalities and more.’
Joao Breda, Head, WHO European Office for Prevention and Control of Noncommunicable Diseases
The scope of the assessment is wide-ranging, with ten policy and programme indicators, including national leadership, Baby Friendly hospital and community practices, marketing controls on breastmilk substitutes, health professional training, emergency preparedness and monitoring. There are also five feeding practices indicators, such as exclusive breastfeeding for 6 months, a WHO recommendation.
The original assessments were all carried out using the World Breastfeeding Trends Initiative (WBTi), a tool first developed in 2004 by the International Baby Food Action Network (IBFAN) but only launched in Europe in 2015. It requires collaboration with relevant organisations within a country on assessment scores, gaps identified and recommendations for improvements. The Report highlights good practice, enabling countries to learn from one another.
˝Success …rests first and foremost on achieving political commitment at the highest level and assembling the indispensable human and financial resources.’
WHO Global Strategy 2003
If governments, other policymakers, hospitals and community services, public health departments, institutions that train health professionals, and others, adopt the report recommendations, it will enable more mothers to initiate and continue breastfeeding, strengthening the health of the population for the future.
The WBTi European Working Group, led by Dr. Irena Zakarija-Grkovic of Croatia, produced the Report and comprises coordinators from European countries which have carried out a WBTi assessment. The production of the report was supported by the Croatian Ministry of Health and UNICEF Croatia.
Maternal Mental Health Day is on the first Wednesday in May, which this year was 6th May. A group of organisations has launched a new survey to try to capture parents’ experiences in the context of a global pandemic and social distancing. If the survey can be distributed widely to parents with a baby/child under 2 year, or are pregnant, to gather the views of parents of a range of ages, ethnicities and experiences, the data will be particularly useful.
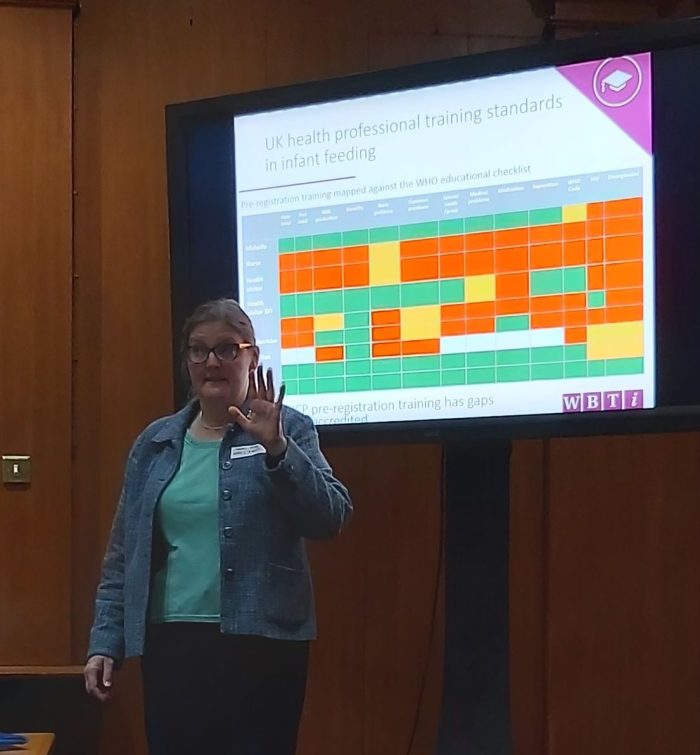
2016 WBTi Report on the UK : see Indicator 5 for health professional training, with the main summary table in Part 1 and details for individual professions in Part 2.
Working with public services to support families better with infant feeding and developing close loving relationships through training and accreditation
Doctors have an important role to play in supporting mothers who want to breastfeed.
A continuing theme of the WBTi UK work is improving medical training in infant feeding such that all, not just some, doctors have sufficient knowledge and understanding of breastfeeding to protect the decisions of mothers who want to breastfeed. Enabling more mothers to continue breastfeeding would improve infant and maternal health, reduce NHS costs (Renfrew et al) and reduce the number of GP appointments (Pokhrel et al, 2015).
Supporting Mothers Who Breastfeed, by Patricia Wise. E-book downloadable from the WBTI website
Georgie BHS and Dani Phillipson from the Parenting Science Gang, which runs citizens’ science projects using mothers to collect evidence, spoke next. They described the breastfeeding and healthcare experiences project (inspired in part by the WBTi findings on health professional training) with its subsidiary small project of 8 interviews looking at healthcare professionals’ own experiences of breastfeeding on their professional practice. From the themes identified, PSG has produced MILK cards to guide health professionals:
Mothers’ voices matter
Investigate common issues, but also
Look for underlying causes§
Know where to find information
GP Dr. Terri Lovis (seen in banner photo above) described how the GP Infant Feeding Network (GPIFN), initiated by Dr. Louise Santhanam, was set up as a pharma free network to improve the quality of support in infant feeding with the work provided voluntarily. The website is a comprehensive educational resource for primary care and there is partnership with the Hospital Infant Feeding Network (HIFN). Additional achievements include working collaboratively with IMAP (International Milk Allergy in Primary Care Guidelines) to produce the 2019 version and bidding successfully with PHE and Surrey Heartlands to train Infant Feeding champions across Surrey (as Norwich already does).
Dr Natalie Shenker from the Human Milk Foundation
The fascinating keynote presentation was by Dr. Natalie Shenker on Doctors and Breastmilk, and included the initiation of the Human Milk Foundation in 2017 and the work of the Hearts Milk Bank, which she co-founded with Gillian Weaver. The Milk Bank is involved in research as well as providing pasteurised donor milk.
The challenge is how to enable all medical students, trainees and qualified doctors to acquire an adequate minimum standard in infant feeding knowledge and skills. Yes, there is a huge amount that they need to know in total but being breastfed as an infant can make such a difference to the health of baby and mother (not to mention the environmental sustainability of breastfeeding!) that it is crucial to include. Some examples of what is already being done to help achieve this:
Imperial College Medical School is running a programme in which medical students are allocated to follow a mother from the end of pregnancy until the child is 3 years old.
Norwich CCG has a GP Champion in Infant Feeding scheme, which Surrey Heartlands is also rolling out, in which the champion receives training and disseminates the learning throughout the practice.
Imagine if all medical schools ran such a programme and all GP practices had a breastfeeding champion!
Banner photo: Dr. Terri Lovis
Patricia Wise is the author of ‘Supporting Mothers Who Breastfeed: A Guide for Trainee and Qualified Doctors’. She is an NCT Breastfeeding Counsellor and tutor, and a member of the WBTi UK Steering Group