National governmental leadership in the UK and devolved nations could make a significant difference by making legal, policy and structural changes. These would filter down through every level of society to show ACTION for the shared responsibility of protecting and supporting every child’s human right to have the best start in life.
There have been Calls for Action before with slow or indifferent responses. The new Health Security Agency has an opportunity to fulfil its responsibility to the health of England’s population by making positive changes NOW.
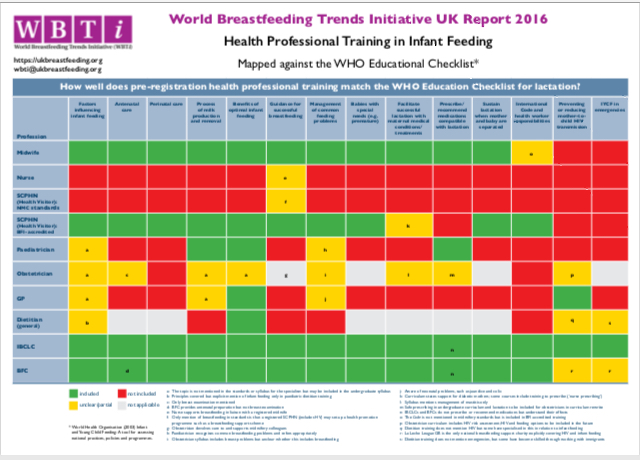
A WBTi report identifies gaps and makes recommendations. The UK report in 2016 reported that, for Indicator 1, which covers National policy and whether there is an associated programme and coordination, the scores from the assessment were:
England 1
N.I. 10
Scotland 10
Wales 4
Sadly, the situation remains unchanged in England. It is TIME to invest and implement recommendations, which are supported by the broad alliance of infant feeding agencies who have come together to speak, with one voice, on behalf for all new families’ futures in this uncertain world.
Establish a structure for monitoring implementation of the Code and that action is taken against violations.
Create a multi-sectorial, funded lead, for Infant Feeding in England with a strategy and route to share best practice.
Ensure full and equitable access to skilled support for every new mother.
Build in improvements to monitoring and collection of data.
All these improvements would help protect the breastfeeding dyad much better and move much closer to the vision of all UK families experiencing a society that is supportive of breastfeeding with ready accessible skilled support available whenever is needed.
Author: Clare Meynell RM (rtd) IBCLC
Clare trained as a child & general nurse before a long career as a midwife and infant feeding lead. more than 25 years. Clare has also led La Leche League peer support training sessions in her local community. Currently, with Helen Gray, Clare jointly coordinates the UK WBTI working group and co presented the first report for the UK in Parliament in November 2016.
Working with her colleagues she hopes to create “Actions for Change”, through the WBTi report recommendations, so the next generation of mothers are enabled to achieve their personal breastfeeding goals and that society better values the health giving properties of human milk as the physiologically normal food for babies.
For Day 2 of WBW we are very pleased to have a guest blog by Health Visitor and Clinical Research Fellow Dr. Sharin Baldwin.
Breast milk provides the ideal nutrition for infants and its associated benefits to the infant, mother and the wider public health are well documented. Traditionally breastfeeding promotion and advice have been targeted at expectant and new mothers, with an aim to increasing breastfeeding rates in infants. In recent years it has been acknowledged that partners play an important role in supporting women’s decision to breastfeed, while also providing practical and emotional support with the continuation of breastfeeding. Research highlights the important role of fathers in promoting and supporting their partners with breastfeeding (Tohotoa et al., 2011; Datta et al., 2012; Sherriff et al., 2014; Hansen et al., 2018), but in practice fathers continue to report inadequate levels of information and support from health professionals. Training for health professionals therefore should consider men’s needs relating to breastfeeding promotion and support, as well as women’s.
New fathers have often reported finding their partner’s breastfeeding experiences to be much more difficult than they had originally anticipated, with many not knowing how to help or support their partner with breastfeeding when they experienced difficulties (Baldwin et al, 2018; 2019). This is where health professionals can really make a difference. They can help educate and prepare expectant fathers better during the antenatal period by providing them with ‘realistic’ information about the time it may take for their partner to establish breastfeeding. It is also important to highlight some of the breastfeeding challenges they may face in early parenthood and what strategies or support are available to overcome them. This will help men to develop more realistic expectations of the processes involved with establishing breastfeeding and make them feel more empowered to support their partner when faced with any difficulties.
While fathers may not be able to be directly breastfeed their babies, they need to know that they play a crucial role in making breastfeeding a success. They can provide practical support to their partners through helping with household duties, giving them a massage, allowing them to rest, making meals and drinks for them, and giving them emotional support through regular praise, reassurance and encouragement. Good levels of breastfeeding support are likely to make the process easier and more enjoyable, while giving women the confidence to continue breastfeeding for longer. Fathers’ involvement in breastfeeding not only has the potential to increase breastfeeding rates and duration, but also contribute to better outcomes for babies, mothers and the wider public health agenda. So, let’s not forget about including fathers when having those crucial discussions and training about breastfeeding!
Baldwin, S., Malone, M., Sandall, J., Bick, D. (2018) Mental health and wellbeing during the transition to fatherhood: a systematic review of first-time fathers’ experiences. JBI Database of Systematic Reviews and Implementation reports, 16(11):2118–91.
Baldwin, S., Malone, M., Sandall, J., Bick, D. (2019) A qualitative exploratory study of UK first-time fathers’ experiences, mental health and wellbeing needs during their transition to fatherhood. BMJ Open 2019;9:e030792. doi:10.1136/bmjopen-2019-030792 https://bmjopen.bmj.com/content/9/9/e030792.info
Datta, J., Graham, B., Wellings, K. (2012) The role of fathers in breastfeeding: decision-making and support. British Journal of Midwifery, 20(3):159–167.
Hansen, E., Tesch, L., Ayton, J. (2018) ‘They’re born to get breastfed’- how fathers view breastfeeding: a mixed method study. BMC Pregnancy and Childbirth, 18:238 https://doi.org/10.1186/s12884-018-1827-9
Sherriff, N., Hall, V., Panton, C. (2014) Engaging and supporting fathers to promote breast feeding: A concept analysis. Midwifery, 30: 667–677.
Tohotoa, J., Maycock, B., Hauck, Y.L., Howat, P., Burns, S., Binns, C.W. (2009) Dads make a difference: an exploratory study of paternal support for breastfeeding in Perth, Western Australia. International Breastfeeding Journal, 4: 15. http://dx.doi.org/10.1186/1746-4358-4-15
Author:
Dr. Sharin Baldwin PhD, MSc, PG Dip, BSc (Hons), HV, RM, RN, QN, FiHV, IHV Research & PIMH Champion
NIHR Clinical Research Fellow, University of Warwick
Clinical Academic Lead (Nursing and Midwifery), London North West University Healthcare Trust
The theme of International Women’s Day (IWD) this year is Choose to Challenge. The IWD website explains: ‘from challenge comes change. So let’s all choose to challenge.’ However, challenging can take courage. It’s preferable if it can be done in a way that shows understanding – as a critical friend – rather than confrontational, as the latter can trigger a defensive reaction that blocks change.
The WBTi report in 2016 showed that considerable change is needed to support breastfeeding better in the UK. This is part of achieving a larger picture in which babies are valued and there is no discrimination against women. In part it is a human rights issue. ‘Women have the right to accurate, unbiased information in order to make an informed choice about breastfeeding … and they have the right to … appropriate conditions in public spaces for breastfeeding which are crucial to ensure successful breastfeeding.’
IWD is also an opportunity to celebrate women’s achievements. How amazing it is that the female body naturally produces milk that is just right for her baby – in nutrition and immunity – and the milk changes to match her baby’s changing needs. But childbearing is no reason to discriminate against women in a different role – in the workplace. And, turning to economics, GDP does not include unpaid work or the production of human milk, leading to the anomaly that increased formula sales increase GDP and greater production of valuable human milk reduces it!
What are some ways of challenging?
Challenging government
This could involve commenting on draft laws when they are out for consultation and/ or supporting amendments, as is happening with the Domestic Abuse bill currently going through Parliament, which currently overlooks the impact on babies. Writing to your constituency MP to raise awareness of an issue is another way. The UK Regulations on Infant Formula and Follow-on formula are still considerably weaker than the WHO International Code and are not enforced, but it is also useful to consider when effort to challenge is most likely to be productive. Revised guidance that was due to come into force in February 2021 has been delayed by a year, but the pandemic has led to some government department timescales slipping.
The original guidance from Public Health England about vaccinations for breastfeeding mothers was discouraging but members of national breastfeeding support organisations and the GP Infant Feeding Network (GPIFN) challenged this, and the guidance was improved. The guidance now states that, although there are no data, ‘vaccines are not thought to be a risk to the breastfeeding infant, and the benefits of breastfeeding are well known.’
Another opportunity is provided by public consultations on NICE guidance when new guidance is produced or existing guidance is reviewed, as for the Postnatal Guidance in the autumn of 2020.
Commenting on articles or writing them
Recently, several letters were sent to the editor of ‘New Scientist’ following publication of an article which misunderstood why infant formula is not made available at Food Banks, despite Unicef UK already having produced an information sheet.
An article by Naomi Joffe, Flic Webster and Dr Natalie Shenker in 2019, Support for breastfeeding is an environmental imperative, was published in the British Medical Journal, helping to raise awareness among the medical profession.
Challenging myths and poor information on social media sites
Misinformation can spread quickly so it is important, sensitively, to try to prevent its spread.
Challenging supermarkets/ pharmacies and advertising
This could be about special offers in stores that break the UK Regulations; finding the courage to raise this with the manager raises awareness and hopefully lead to change. Advertising that is misleading can be reported to the Advertising Standards Authority. There is relevant information on the Baby Feeding Law Group (BFLG) website.
Representing and supporting parents
This might, for example, be working to improve practice by representing service users on a Maternity Voices Partnership or local Breastfeeding Strategy group. It could also involve empowering a mother who has received poor care to make a complaint.
Trained supporters educating and helping parents help to spread evidence-based information and challenge myths. Mothers can face a variety of barriers to achieving their breastfeeding goals – being separated unnecessarily from their baby, poor and conflicting advice, undermining comments, over-cautiousness when medicines are prescribed……..Enabling them to overcome such barriers can be like starting ripples in a pool that then influence others positively.
Looking to the future
The pandemic has shown that people with underlying health issues such as obesity or diabetes, which are linked to a poorer immune system, are at greater risk of severe Covid-19. Breastfeeding helps babies establish a balance gut microbiome which in turn aids the development of a strong immune system.
With global warming and the overuse of the Earth’s resources, it is essential to reduce carbon emissions and live much more sustainably. Breastfeeding is the most locally produced food there can be. In contrast, the manufacture and use of formula milks leaves significant carbon and water footprints.
Thus supporting mothers to breastfeed for as long as they wish helps in very significant ways – improving population health and protecting the Earth. In addition, mothers who achieve their breastfeeding goals are less likely to suffer mental ill-health or have feelings of guilt, loss and failure. Infants have a right to the highest attainable standard of health and they also gain because they receive breastmilk and experience the nurturing effects of breastfeeding for longer.
Breastfeeding has been shown in many studies to be linked to better health in babies and mothers. As breastfeeding is the physiologically normal way for infants to be fed, it is more accurately stated that not breastfeeding is associated with poorer levels of health. This is not surprising as infant formula only provides the basic nutrition a baby needs (proteins, carbohydrates, fats, minerals and vitamins) but breastmilk is an amazing fluid with over 300 different components, as shown here. It includes growth factors, hormones, enzymes and anti-microbial factors as well as nutrients, and varies in exact composition according to the needs of the baby. It is therefore unique for each mother at each moment in time.
Knowing how amazing human milk is can help a mother have determination to overcome breastfeeding difficulties but it can also feel like pressure. What she needs is access to accurate information and suggestions, offered in a caring way after listening to her particular situation. That means that everyone who has contact with new mothers needs to have sufficient knowledge and person-centred communication skills.
Rachel describes her experiences of giving birth and breastfeeding during lockdown.
Rachel’s story
“During my three years of trying to conceive and infertility treatment I often fantasied about the closeness of holding my baby and feeding them. When I was lucky enough for my IVF to work, I moved on from worrying about if I could have a baby to if I could breastfeed. My mum assured me it was easy for her but her emphasis on its importance felt like further pressure. Many of my friends had stressful experiences and got medical advice that they needed to supplement with formula. Towards the end of my pregnancy I got a phone call from the hospital to explain all the benefits of breastfeeding and recommended I harvest colostrum at 37 weeks. I tried this but couldn’t get even a drop which further made me doubt my ability to breastfeed.
My baby was born in May during the pandemic, so I wasn’t allowed a water birth and my husband was only allowed in during active labour. This meant when I was 3 cm dilated and having intense contractions he had to wait outside the hospital in the car. They refused to check my dilation again for five hours due to infection risk and left me alone. When around 4 hours later I felt the urge to push I convinced the midwife to stay and help. When they could see my baby’s head, I was allowed to telephone my husband and ask him to come. My husband was there for the last 10 minutes but it had been a lonely labour due to COVID-19 without most of the plans I had made that involved a birthing partner.
After the birth the level of support dramatically increased with my husband and midwives all keen to help. My baby was placed on my chest and knew instinctively how to feed and stayed on for hours, it was amazing. I continued to use the gas and air for this first feed as for me the breastfeeding gave me very strong period-like contractions. After this first feed, I no longer had the period-like contractions, but my nipple started to become sore. I decided to stay a night in the hospital for some extra breastfeeding and baby care support, as most face-to-face community support wasn’t available at that time. The midwives repeatedly showed me how to improve my breastfeeding latch throughout the night.
The first breastfeed
Five days after the birth I saw the doctor for routine checks. The doctor calculated my baby had lost 7% of her baby weight (which I believe is normal) but she still asked if I was feeding my baby enough. She asked if my breasts were soft and empty after feeding. At this point my milk hadn’t come in so I didn’t understand the doctor even when I asked her to explain more and had to say no they don’t empty. She also had a look at my nipples and said they were cracked so insisted I must use a nipple shield and wouldn’t discuss any other options. After the appointment I cried in the car park that I couldn’t feed her properly and was failing as a mother. On the way home we rushed to shop for nipple shields (the first shop I had been in since the start of lockdown). I couldn’t get the shields to work and my internet research in some cases strongly warned against their use. I didn’t know what to do so rang my mum and then the hospital. I spoke to a lovely midwife who reassured me and said I didn’t have to use nipple shields and that my nipples could heal with continued feeding.
Due to COVID-19 I had a triage phone call with the health visitor the following week, to assess if I needed a visit. She decided that I needed a visit to weigh my baby and gave me leaflets about local breastfeeding support as my nipples were still painful during feeding. There was no face-to-face support available, but I had a video call with the breastfeeding advice line and joined a virtual group. These calls have been great for giving me personalised support to improve my breastfeeding latch so that feeding is no longer painful, listen to my concerns and build my confidence. It is also very convenient as I don’t need to leave my home for it.
My baby is now almost 10 weeks old and breastfeeding is going well. I can feed her watching TV, half asleep in the dark or on the bench in the park without much effort and with no discomfort. I am also pleased not to need to warm up formula as that might be harder when cafes and other facilities are closed due to COVID-19. I love being close to my baby during breastfeeding and being able to provide what she needs.”
Thank you very much, Rachel, for sharing your story.
The year 2020 has seen us facing unprecedented multiple crises and emergencies:
· COVID19
· The Climate Emergency
· A crisis propelling equity, racial and social justice to the forefront through #BlackLivesMatter
The global theme of World Breastfeeding Week 2020, “Support breastfeeding for a healthier planet,” is a focus on the Climate Emergency, and the impact of infant feeding on our environment and the planet.
#SupportBreastfeedingforaHealthierPlanet
We can all think of so many ways that breastfeeding is good for the planet – no food miles at all, no pollution or litter from manufacturing or distribution, a very small carbon footprint to feed a breastfeeding mother rather than a herd of cows! Most mothers in the UK want to breastfeed, and mothers are already doing the best they can. It is really our governments and policy makers who need to wake up to this, and they who should provide the policies and programmes that families need to breastfeed. And it is our governments who have the responsibility to plan a “green recovery” from COVID19, so that we can return to a healthier world for everyone.
“Overall, breastfeeding for six months saves an estimated 95-153kg of CO2 equivalent per baby”. This comes from an 2019 BMJ editorial by Joffe, Webster and Shenker called Support for Breastfeeding is an environmental imperative. Yet only 1% of babies in the UK are exclusively breastfed for six months (PHE).
Most formula is based on cows’ milk, and dairy farming has a significant burden of greenhouse gases, both carbon and methane. (GreenFeeding). Processed, powdered formula milk has a large water footprint as well – up to 4700 litres for every kg of milk powder! (IBFAN)
Bottle feeding also requires multiple plastic bottles and teats, as well as fuel to boil water, sterilise equipment, and store formula safely. Bottle feeding in hospitals creates waste, as described by Becker and Ryan-Fogarty in the BMJ.
One example of a government policy that could support families and reduce the need for these would be breastfeeding breaks at work, and childcare close by. This would enable mothers to feed their children themselves, without the additional burden of expressing and storing their milk. Going back to work was cited as one of the main reasons that women stopped breastfeeding early.
There will always be a need for formula and bottles for those babies who cannot be breastfed. But most mothers in the UK do want to breastfeed, and it is the responsibility of our government, of our health system, and our local authorities, to provide the policies and programmes to enable women to continue breastfeeding as long as they want to.
With breastfeeding support under strain, service providers propose plan to tackle inequalities
This World Breastfeeding Week (1-7 August 2020), #WBW2020 and #GreenFeeding, we are calling on the UK government to address the fragility of breastfeeding support services.
Our organisations have seen first-hand how the Covid-19 crisis has exposed the fragility of infant feeding support available for women, parents and families.
Over the past few months, the need to support babies and families has escalated and support services have been stretched beyond anything in our experience.
Existing variations in provision for infant feeding support have increased as services have been cut, health visiting teams redeployed and provision moved online, leading to unknown outcomes on infant nutritional health, worsening maternal mental health and widening health inequalities.
Tremendous efforts from the NHS and Third Sector organisations, including many volunteers on the National Breastfeeding Helpline and other charity-run helplines, along with swift adaptation to offer online support, have provided many families with support but this is not sustainable without a longer term strategy.
Meanwhile, the need to protect infant and young child feeding in pandemic emergencies has not previously been considered and has been entirely missing from the Scientific Advisory Group for Emergencies’ reports.
Investing in the health of new families, including supporting and protecting breastfeeding and supporting safe and responsive formula or mixed feeding, enables children not just to survive, but to thrive.
Rebuilding infant feeding support for communities after Covid-19 and giving important attention to the needs of mothers and children from Black, Asian and minority ethnic backgrounds will help tackle inequalities.
Infant feeding is a critical component of first 1001 Days and Early Years Health
We welcome the appointment of Andrea Leadsom MP as the Government’s Early Years Health Adviser and the announcement of a review at a time when infant feeding support services for women, parents and families have been stretched to an unprecedented degree.
Protecting breastfeeding and ensuring safe and responsive formula and mixed feeding during those first 1001 days would make a significant contribution to reducing inequalities in health. As a result, it also upholds the work of the NHS and helps build a healthier population.
While COVID-19 has undoubtedly placed a strain on support systems, it has also highlighted a huge omission in UK policy on planning for the care and feeding of infants and young children in case of emergencies, leaving our youngest members of society vulnerable.
While the benefits of breastfeeding are well-evidenced, merely stating these benefits does not ensure breastfeeding is protected or supported. At a time of global health crisis, and increasing recognition of the impact of human behaviour on the health of our planet, support for breastfeeding is also an environmental imperative.
10-point Infant Feeding Action Plan to address Inequalities
We call on the UK government to adopt the following 10-point Infant Feeding Action Plan below which has a particular focus on working to reduce inequalities:
For the new Government Early Years Advisor to appoint a permanent, multi-sectoral maternal, infant and young child nutrition strategy group to implement a national strategy to support good nutrition across the first 1001 days.
To commission and sustainably fund universal, accessible, confidential breastfeeding support delivered by specialist/lead midwives, health visitors and suitably qualified breastfeeding specialists, recognising the role of charitable organisations and community groups and their strong links with communities.
To ensure there are children’s centresor family hubs, disproportionately located in areas of disadvantage, offering joined-up universal services that include breastfeeding peer support, guidance on the introduction of solids and eating well in the early years.
To ensure that health visiting services are properly funded and the number of health visitors increased to ensure consistent timely nutritional support for all families to support good maternal and infant mental and physical health.
To integrate planning to support infant and young child feeding in emergencies into legislation, the Civil Contingencies Act, and Local Resilience Forums across the country.
To recognise the importance of breastmilk for preterm and vulnerable babies and the need for equitable access to donor breastmilk for these babies through the establishment of a fully funded regional donor milk banking service.
To implement the Unicef UK Baby Friendly Initiative across community, hospital and neonatal services, building on the recommendation for all maternity services to be accredited in the NHS Long Term Plan.
To make it a statutory right of working mothers to access a private space and paid breaks to breastfeed and/or express breastmilk and manage its safe storage.
To support the commitment to re-instate the quintennial Infant Feeding Survey which builds on data previously collected every five years since 1975, most recently in 2010.
To protect babies from harmful commercial interests by bringing, as a minimum, the full World Health Organisation International Code of Marketing of Breastmilk Substitutes into UK law and enforcing this law.
The Breastfeeding Network Association of Breastfeeding Mothers NCT La Leche League GB HENRY Institute of Health Visiting Best Beginnings Human Milk Foundation Local Infant Feeding Information Board Lactation Consultants of Great Britain World Breastfeeding Trends Initiative UK Hospital Infant Feeding Network GP Infant Feeding Network UK Association of Milk Banking Diversity in Infant Feeding Better Breastfeeding Nursing Matters Save Time Support Breastfeeding Swansea University Breastfeeding Twins and Triplets
The year 2020 has seen us facing unprecedented multiple crises and emergencies:
COVID19
The Climate Emergency
A crisis propelling equity, racial and social justice to the forefront through #BlackLivesMatter
The global theme of World Breastfeeding Week 2020, #WBW2020 and #GreenFeeding, “Support breastfeeding for a healthier planet,” is a focus on the Climate Emergency, and the impact of infant feeding on our environment and the planet.
When the novel coronavirus hit it reminded us that we are all linked, one people on one planet.
Breastfeeding and COVID-19
Some of those people were breastfeeding mothers and babies. At first, medical protocols for isolating COVID+ patients dictated that some mothers and babies were separated. Slowly the evidence accumulated that breastmilk itself did not appear to transmit the virus, and in fact antibodies to COVID19 began to be found in mothers’ milk. Now there are even research projects investigating whether the antibodies to COVID-19 in breastmilk could be used to protect others!
In the UK, the Royal Colleges who work with mothers and babies, led by the Royal College of Obstetricians and Gynaecologists (RCOG) and the Royal College of Midwives (RCM) quickly began to produce joint guidance, updated weekly. This was hosted on the RCOG website and became a global point of reference.
Coronavirus (COVID19) infection and pregnancy: this clinical guidance contains their influential recommendations on keeping mothers and babies together in hospital after birth, whether or not the mother is COVID+, and their recommendation that staff support the mother to breastfeed or express her milk for her baby, unless the mother is too ill. These recommendations have influenced health policy around the world, keeping many mothers and babies together worldwide.
A useful Q&A page of information for women and their families, written in plain language.
Guidance for antenatal and postnatal services during the evolving coronavirus (COVID19) pandemic. This includes some information on the management of breastfeeding in the community, including the following : “Remote support by third-sector organisations will be invaluable to provide support for breastfeeding, mental health and early parenting advice.”
The World Health Organisation has produced a steady stream of updates and resources emphasising the importance of breastfeeding during the COVID crisis. This includes:
a media briefing on the 12 June at which the Director-General stated:
“WHO has also carefully investigated the risks of women transmitting COVID-19 to their babies during breastfeeding.
We know that children are at relatively low-risk of COVID-19, but are at high risk of numerous other diseases and conditions that breastfeeding prevents.
Based on the available evidence, WHO’s advice is that the benefits of breastfeeding outweigh any potential risks of transmission of COVID-19.
Mothers with suspected or confirmed COVID-19 should be encouraged to initiate and continue breastfeeding and not be separated from their infants, unless the mother is too unwell.
WHO has detailed information in our clinical guidance about how to breastfeed safely.”
We recommend that mothers with suspected or confirmed COVID-19 should be encouraged to initiate and continue breastfeeding. From the available evidence, mothers should be counselled that the benefits of breast-feeding substantially outweigh the potential risks of transmission.
In the UK, breastfeeding services suffered as midwifery and health visiting staffing levels were reduced by illness and self isolation, some staff were redeployed to labour ward or public health, childrens’ centres and breastfeeding support groups were closed. Families were discharged with their new baby to go home to a changed world, isolated in their home. Most health professional contacts were now virtual, and there were few opportunities to have baby weighed or seen in person, so parents were left on their own to figure out if their baby was doing well.
In areas like Brighton, with a strong, integrated commissioned NHS breastfeeding support programme, with a well embedded, large trained peer support programme and where there is a specialist NHS IBCLC clinic for complex problems, all the NHS support simply moved online. Once the technical side of this was worked out, breastfeeding support was still there for those who needed it.
In other areas, that depended on health visitors alone to deliver all the breastfeeding support, where there was no peer support commissioned and no specialist clinic staff, once the childrens’ centres were closed and many health visitors redeployed to other public health roles during the COVID-19 crisis, there might be one infant feeding lead health visitor left in the whole community.
Across the country, breastfeeding organisations and breastfeeding supporters sprang into action. Calls to the National Breastfeeding Helpline rose significantly, and trained volunteers turned out in droves. NCT moved their antenatal classes online, La Leche League local groups and NCT breastfeeding support groups moved onto Zoom, and IBCLCs set up remote consultations. A new app was trialled through the NHSX TechForce19 competition, Peppy Baby, in collaboration with Lactation Consultants of Great Britain and NCT, providing free access to online support groups and even video consultations for specialist breastfeeding help and mental health support. Suddenly there was online breastfeeding support available somewhere, every day of the week.
This had some advantages: mothers could join a Zoom meeting with their baby, still in bed. No one had to travel to get help. But some families had complex situations that did need face to face support, and it could be a challenge to find a specialist who could provide face to face support, or a tongue tie clinic that was still open.
Some families were able “nest” in isolation, with both parents home and no visitors, and flourished. Others struggled without face to face contact, without weight checks for baby, or struggled with their mental health. It will be hard to unpick the outcomes, as in many areas the usual health visitor checks were no longer taking place in person, so there are many gaps in the data. For instance, in some areas, no-one collected breastfeeding rates at 6-8 weeks, so it will be difficult to see the impact of COVID-19 on breastfeeding there.
It is vital that we all call on our local authorities, our CCGs and our Local Maternity Systems to rebuild a stronger network of skilled breastfeeding support as we come out of this first COVID-19 crisis – we must be more prepared for the next one.
This is the start of World Breastfeeding Week 2020, which runs from the 1st to the 7th August. WBW is a global campaign to raise awareness and galvanise action on themes related to breastfeeding and commemorates the 1990 Innocenti Declaration. Since 2016, WBW has been aligned with the United Nations’ Sustainable Development Goals.
Breastfeeding can be hard in the early weeks under normal circumstances, adjusting to meeting the needs of a vulnerable human being, including urgent frequent feeding, and the tiredness that results from being on call 24 hours a day, 7 days a week. If feeding is painful it feels even harder. That is why having skilled breastfeeding support readily available, for any mother that needs it, is so important. Breastfeeding usually becomes much easier and more enjoyable as the weeks pass, especially if worries about painful feeds or milk supply or difficulties due to causes like tongue-tie are resolved, and is helped by babies tending to have more spaced and shorter feeds.
This year Covid-19 lockdown has been an added complication, particularly for new families as they have minimal face-to-face contacts.
What have the challenges and highlights been for you? You can share your experiences using the Leave a Reply box below.
A new study by trainee doctor Kirsty Biggs and senior colleagues has shown that 97% of the 411 medical students who responded to a survey are uncertain of their practical skills to support new mothers with breastfeeding, such as helping with latch issues, although the overall benefits of breastfeeding were moderately well-known. Yet most students (93%) perceived doctors to have an important role in supporting breastfeeding and the same percentage requested further breastfeeding education.
Over 80% of the respondents had a career interest in obstetric and gynaecology, paediatrics and/or general. While the sample was only around 1% of UK medical students, and only one-quarter of the students responding were male, it’s a very clear message that breastfeeding education overall is not adequate.
Around 80% of the 32 UK medical schools eligible responded to their part of the survey and results indicate that only 70% of medical schools provide compulsory breastfeeding education.
WBTI’s findings and vision
The WBTi UK report in 2016 indicated that medical curricula have many gaps with regard to breastfeeding, and Biggs’ study confirms that the students themselves find it inadequate. WBTi UK’s vision is that all doctors have sufficient training in infant feeding to protect the decisions of mothers who want to breastfeed.
How can the situation be improved? High level standards and Unicef BFI learning outcomes
The General Medical Council provides broad guidelines for undergraduate curricula in its Outcomes for Graduates document and each medical school devises its own curriculum to fit the guidelines. For example, the expectation under the Outcomes Health promotion and illness prevention section is: ‘Newly qualified doctors must be able to apply the principles, methods and knowledge of population health and the improvement of health and sustainable healthcare to medical practice’. Unicef UK Baby Friendly Initiative’s learning outcomes for several professions, including medical students, published in November 2019 are highly relevant to improving curricula and accompanying resources are being developed.
RCPCH curriculum – an encouraging sign
Medical training is long, with undergraduate, Foundation and then specialty training. The RCPCH (Royal College of Paediatrics and Child Health) states as part of its activity to promote breastfeeding: ‘The RCPCH training curriculum for General Paediatricians and all paediatric subspecialties requires training to understand the importance of breastfeeding and lactation physiology, be able to recognise common breastfeeding problems, have knowledge of formula and complementary feeding, and be able to advise mothers or refer for support.’
Mentioning infant feeding in guidance to doctors to encourage including it in consultations is also important. GP Louise Santhanam (founder of GPIFN) is the lead author of Postnatal Maternal and Infant careduring the COVID-19 Pandemic: a Guide for General Practicethat was recently added to the RCGP website. This clarifies that 6-8 week checks need to continue despite the Covid-19 pandemic and that infant feeding should be a routine clinical consideration.
Thus plenty of resources are available but doctors are busy people. While some really understand the importance of protecting breastfeeding, and know how to – such as signposting mothers to local skilled help – the challenge is how to bring this into every medical student’s training.
If you know anyone at medical school, it would be really useful if you can let them know about Kirsty Biggs’ study.
The WBTi UK team are proud to be part of producing this joint statement calling for our next government to make breastfeeding a priority in setting the agenda to prioritise the early years of life.
The new government needs to prioritise the first 1001 days of a child’s life, from conception to age two, to enable children to survive and thrive. How an infant is fed and nurtured strongly influences a child’s future life chances and emotional health. Importantly, if a woman breastfeeds there are substantial health benefits for her – having impacts onher future long after breastfeeding has stopped.
Independent, practical, evidence-based information and support is essential for every family. Supporting women with breastfeeding can go a long way to protecting children and mothers from a wide range of preventable ill health, including obesity and mental health problems.
This window of opportunity cannot be missed for the future health outcomes of mothers and the next generation. In addition to well documented health outcomes, supporting breastfeeding will also contribute to a stronger economy – potential annual savings to the NHS are estimated at about £40 million per year from just a moderate increase in breastfeeding rates.
Support for breastfeeding is also an environmental imperative and recognition of the contribution breastfeeding can make to avoiding environmental degradation should be a matter of increasing global and political attention.
In the UK, the majority of women start to breastfeed but breastfeeding rates drop rapidly – our continuation rates are some of the lowest in the world and are even lower amongst women living in deprived areas, where increasing rates could make a real difference to health inequalities. Support for all women, parents and families with breastfeeding falls short of what is wanted and needed.
Women tell us they encounter difficulties with the public perceptions of breastfeeding out of the home. Families tell us they are still regularly exposed to conflicting messaging and marketing for formula milks that drowns out advice from healthcare professionals.
Women tell us they receive little to no help with infant feeding and that their health visitors, midwives and doctors often have little training or knowledge about breastfeeding and limited time to support them.
Recent cuts in health visitor numbers and breastfeeding peer support services mean many women may be left without the support they need however they choose to feed their infants.
Despite robust evidence showing that investment in breastfeeding support and protection makes sense, politically breastfeeding has been viewed by governments as a lifestyle choice and so left to parents to work out for themselves. For too many women, trying to breastfeed without support, or stopping before they want to, is deeply upsetting and the situation is made worse by fragmented care, and poor and often conflicting advice from those they are seeking to support them. To ensure an increase in breastfeeding rates, to help reverse obesity rates and to reduce widening health inequalities will require significant investment in breastfeeding.
It is essential that our new government prioritises breastfeeding and invests in its support and protection.
We call on all political parties to commit to the following actions, if elected:
To appoint a permanent, multi-sectoral infant and young child feeding strategy group and develop, fund and implement a national strategy to improve infant and young child feeding practices.
To include actions to promote, protect and support breastfeeding in all policy areas where breastfeeding has an impact.
To implement the Unicef UK Baby Friendly Initiative across community and paediatric services, building on the recommendation for maternity services in the NHS Long Term Plan.
To protect babies from harmful commercial interests by bringing the full International Code of Marketing of Breastmilk Substitutes into UK law and enforcing this law.
To commission, and sustainably fund, universal breastfeeding support programmes delivered by specialist/lead midwives and health visitors or suitably qualified breastfeeding specialists, such as IBCLC lactation consultants and breastfeeding counsellors, alongside trained peer supporters with accredited qualifications.
To maintain and expand universal, accessible, affordable and confidential breastfeeding support through the National Breastfeeding Helpline and sustaining the Drugs in Breastmilk Service.
To deliver universal health visiting services and the Healthy Child Programme by linking in with local specialist and support services.
To establish/re-establish universal Children’s Centres with a focus on areas of deprivation, offering breastfeeding peer support.
To make it a statutory right of working mothers and those in education to work flexibly as required and to access a private space and paid breaks to breastfeed and/or express breastmilk and manage its safe storage.
To commit to resourcing for charitableorganisations who play a key role within the health agenda working at a national and local level to support families and communities with infant feeding.
To support the commitment to undertake an Infant Feeding Survey which builds on the data previously collected in the Infant Feeding Survey 2010 (now discontinued).
To implement the recommendations of the Becoming Breastfeeding Friendly (BBF) study.
CASE FOR ACTION
Breastfeeding benefits all babies, and studies have shown that just a small increase in breastfeeding rates could cut NHS expenditure considerably. It is vital to invest in breastfeeding support in the early months and this will reap rewards in the future that are likely to exceed the initial cash flows associated with putting proper support in place.
A UNICEF reportstates that “no other health behaviour has such a broad-spectrum and long-lasting impact on public health. The good foundations and strong emotional bonds provided in the early postnatal period and through breastfeeding can affect a child’s subsequent life chances”.
Evidence has also demonstrated that a child from a low-income background who is breastfed is likely to have better health outcomes than a child from a more affluent background who is formula-fed. Breastfeeding provides one solution to the long-standing problem of health inequality.
Research into the extent of the burden of disease associated with low breastfeeding rates is hampered by data collection methods. This can be addressed by investment in good quality research.
2. Borra C, Iacovou M, Sevilla A (2015) Maternal Child Health Journal (4): 897-907. New evidence on breastfeeding and postpartum depression: the importance of understanding women’s intentions.
3. Brown, A, Rance J, Bennett, P (2015) Understanding the relationship between breastfeeding and postnatal depression: the role of pain and physical difficulties. Journal of Advanced Nursing72 (2): 273-282
10. National Institute for Health and Care Excellence (2012) Improved access to peersupport NICE, London
11. Rollins N, Bhandari N, Hajeebhoy N, et al (2016) Why invest, and what it will take to improve breastfeeding practices? The Lancet387 491-504
12. Wilson AC, Forsyth JS, Greene SA, Irvine L, Hau C, Howie PW. 1998 Relation of infant diet to childhood health: seven year follow up of cohort of children in Dundee infant feeding study. BMJ. Jan 3;316(7124):21-5.