World Breastfeeding Trends Initiative UK (WBTi)
Uses the WBTi Assessment Tool to score a country’s support for breastfeeding according to 10 key indicators based on evidence-based strategies in the 2003 WHO Global Strategy for Infant and Young Child Feeding:
So far, 97 countries have produced a WBTi report: https://www.worldbreastfeedingtrends.org/
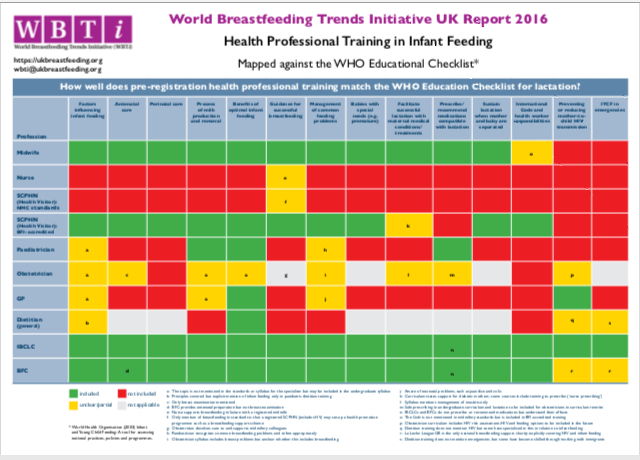
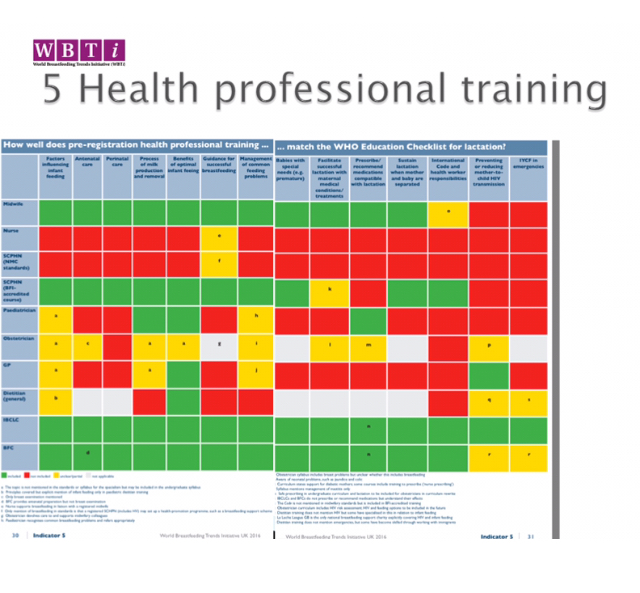
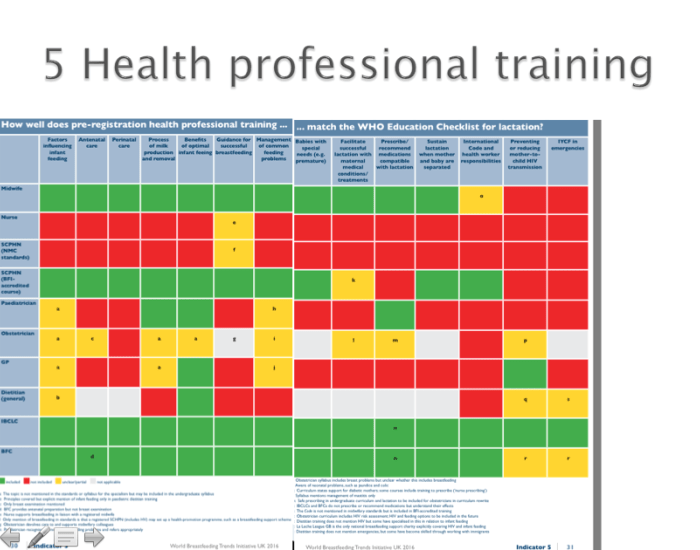
2016 WBTi Report on the UK : see Indicator 5 for health professional training, with the main summary table in Part 1 and details for individual professions in Part 2.
e-book by Patricia Wise of WBTi UK: free downloadable PDF, Supporting mothers who breastfeed: A guide for trainee and qualified doctors
Working to protect all babies by strengthening UK laws on infant feeding in line with UN recommendations
Publications include: Comfort milks, lactose-free infant milks and anti-reflux milks: Why these products should be removed from shop, supermarket and pharmacy shelves
Breastfeeding Network
* Breastfeeding Network Drugs in Breastmilk Information
* Drug fact sheets: https://www.breastfeedingnetwork.org.uk/drugs-factsheets/
New e-learning module Supporting breastfeeding mothers with thrush £30: www.breastfeedingnetwork.org.uk/product-category/training/
e-learning for Healthcare
e-LfH programmes: https://www.e-lfh.org.uk/programmes/
Programmes include: Breastmilk Provision for Preterm and Sick Neonates,
Infant Feeding: supporting education around the implementation of Baby Friendly standards in infant feeding
Public health nutrition charity providing independent information and resources to support eating well from preconception to five years old:
Information on infant milks for health workers
booklets available as free PDFs include: Infant milks in the UK: A practical guide for health professionals:
*GP Infant Feeding Network (GPIFN)
The website is a clinical resource for GPs.
GP Education
iMAP (International Milk Allergy in Primary Care Guideline 2019)
Hospital Infant Feeding Network (HIFN)
The website provides information on supporting breastfeeding in a hospital setting, and there is also a network with a Facebook page.
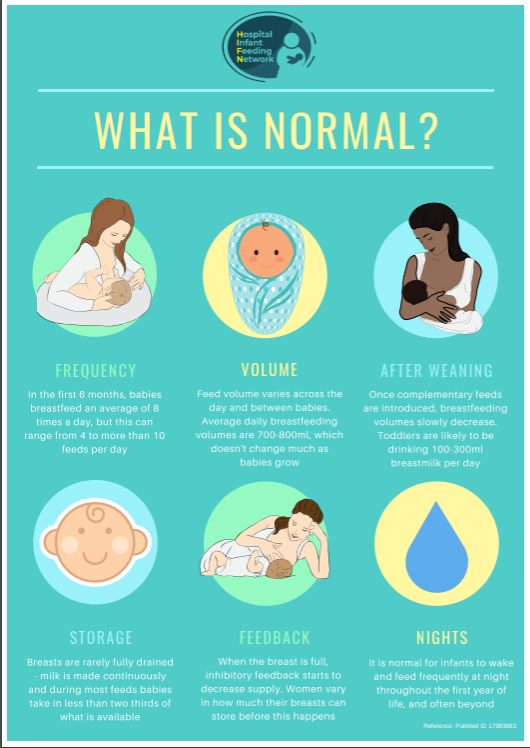
HIFN posters on various aspects of caring for breastfeeding women in hospital
* Don’t stay stop look it up campaign on prescribing for breastfeeding women
Human Milk Foundation
Working to help more families feed their babies with human milk
Hearts Milk Bank: Redefining the boundaries of human milk donation
Lactation consultants of Great Britain (LCGB)
Professional association for International Board Certified Lactation Consultants (IBCLCs)
The crucial role of breastfeeding: supporting mothers with anxiety and depression Handout
Breastfeeding: a vital part of the first 1001 Critical Days. Briefing on the impact of breastfeeding on brain development and infant mental health.
A user-led citizen Science project
Breastfeeding and Health Care Experiences project
Personal Breastfeeding Experience of Health Professionals and Professional Practice
Royal Colleges
Royal College of GPs (RCGP): Breastfeeding Position Statement and link to online resource on breastfeeding
Royal College of Paediatrics and Child Health (RCPCH): Breastfeeding position statement
* UKDILAS: UK Drugs in Lactation Advisory Service
Enquiry-answering service, fact sheets and database on drug prescribing during breastfeeding
Unicef UK Baby Friendly Initiative
Working with public services to support families better with infant feeding and developing close loving relationships through training and accreditation
e-learning packages for GPs and paediatricians
Recommended learning outcomes for different specialisms of healthcare practitioners
Include learning outcomes for medical students
Other resources
Facebook group: Breastfeeding for Doctors Peer Support
* ed. Amy Brown and Wendy Jones (2020) A guide to supporting breastfeeding for the medical profession Routledge
* Wendy Jones (2018) Breastfeeding and Medication Routledge 2nd edition
Key: * relevant to prescribing
WBTi UK Doctors and breastfeeding project 2020
Vision: That all doctors have sufficient training in infant feeding to protect the decisions of mothers who want to breastfeed.