Guest blog by Rosalind Bragg, Director of Maternity Action
Maternity Action’s work centres on protecting the rights of pregnant women and new mothers in the workplace. As a member of the WBTi Core Group, Maternity Action was responsible for gathering most of the information on Indicator 4, “Maternity Protection in the workplace.” They have very kindly allowed us to republish their blog on the current status of breastfeeding in the workplace here during UK National Breastfeeding Weeks.
The original blog can be found on Maternity Action’s website here, along with a range of resources on maternity rights. Follow Maternity Action for updates on their campaigns on this and other important maternity rights.
The right to breastfeeding breaks and facilities is a gap in the policy framework to support new parents to balance work and family responsibilities. The current review of Shared Parental Leave policies is an opportunity to remedy this omission.
On May 15, we presented to the All Party Parliamentary Group on Infant Feeding focusing on Maternity Action’s campaigning against pregnancy and maternity discrimination and the particular challenges facing breastfeeding women in the workplace.
Women in the UK who wish to combine work and breastfeeding have very weak legal protections. Health and safety regulations provide breastfeeding women with the right to a place to rest and to a health and safety risk assessment. While some employers may offer regular breaks to breastfeed or express milk and a private space in which to do so, these are not required by law.
For most women, flexible working requests are the only legal avenue to seek adjustments to their working conditions to facilitate breastfeeding. Employers must seriously consider flexible working requests but can refuse them if they have a good business reason for doing so. On our advice line, we regularly hear from women struggling to negotiate flexible working arrangements on return to work. Employers can, and often do, reject reasonable requests for adjustments to working conditions.
Many of the UK’s trading partners have more constructive approaches to balancing breastfeeding and work. Germany provides paid breastfeeding breaks and facilities while the US provides unpaid breaks. Australia offers an alternative form of protection by prohibiting discrimination on grounds of breastfeeding. These are just a few examples. It is unsurprising that the recent World Breastfeeding Trends Initiative (WBTi) review rated the UK 67th out of 91 countries on its law, policy and programmes that support breastfeeding women.
The current review of the Shared Parental Leave scheme provides an opportunity for Government to reconsider its approach to breastfeeding and work. In 2013, when debates were underway on the new scheme, Maternity Action campaigned for a statutory right to breastfeed on return to work. While this did result in ACAS guidance on the issue, legal protections were not forthcoming.
It is extraordinary that a scheme to encourage parents to share leave from their child’s first weeks should pay so little attention to breastfeeding. The Department of Health recommends exclusive breastfeeding for six months and breastfeeding in conjunction with solid food thereafter. Given the absence of legal protections for breastfeeding women, the vast majority of women who share leave will need to stop breastfeeding prior to return to work. This reduces the number of women prepared to share leave with their partner and also contributes to the UK’s low rate of breastfeeding.
Whether women breastfeed or not, and for how long, is a decision for each woman to make. The role of the law is to remove impediments to breastfeeding, enabling women to make decisions based on their own needs, not the convenience of their employers or other equally irrelevant factors. It is long past time that UK employment law caught up with that of its trading partners and provided formal legal protection for breastfeeding on return to work.
It’s a year since the first WBTi UK report was launched in November 2016 at the Houses of Parliament, giving the first snapshot of the state of breastfeeding support in the UK across the indicators. The report has been used as a basis to advocate for improvements in legislation, in strategy, and in training. It has been shared with MPs, with government ministers, as well as shared widely throughout the breastfeeding community through our website.
During the year, we have hosted monthly blogs on our website, focussing on the various indicators in turn. We have an active social media planning group that publicises the WBTi findings, our blog and activities. The team have also produced numerous journal articles, posters and conference presentations in the UK and beyond. Our talented team of volunteers have also developed a video about our findings. We continue to contribute to ongoing consultations about improving health professional training in infant feeding
Policy Forum: Protecting Infants in UK Planning for Emergencies
On November 28th 2017, we will be holding a policy forum at the Houses of Parliament, in collaboration with Ruth Stirton of the University of Sussex and hosted by Alison Thewliss MP: “Protecting Infants in UK Planning for Emergencies.” This event both celebrates the anniversary of the report and aims to achieve change in Indicator 9, “Infant and young child feeding during emergencies,” which is the policy with the lowest scores across the UK. At present, there are no UK-wide or national strategies addressing the issue and it is not explicitly mentioned in local planning.
Unicef UK Baby Friendly Initiative
The jewel in the crown of breastfeeding support in the UK is the Unicef Baby Friendly Initiative. All maternity units in Scotland and Northern Ireland are accredited and most in England and Wales are working towards it. Many community NHS trusts and boards are also on the ladder towards accreditation. Some neonatal units, university midwifery and health visiting/specialist community public health nursing courses are also involved. All are helping to raise the standards of infant support provided by these health professionals.
Cuts to breastfeeding support around the country
Sadly, the WBTi assessment found that cuts in infant feeding lead posts, drop-ins and peer support programmes as well as specialist services were occurring and this has continued. For example, Blackpool’s service was decommissioned in June and the service in Kent is under threat. It appears that there is an assumption by some commissioners that health visitors can provide a sufficient service. Health visitors do have a responsibility to provide effective support with infant feeding, and should do so at statutory visits and other contacts. However, a significant number of mothers also require specialist support, which needs time as well as skill, and all mothers can benefit considerably from the social support that trained peer supporters can provide. It seems it is not well understood how challenging some breastfeeding situations are and the amount of training required to help effectively in those situations.
Ask YOUR MP to join the Call to Action!
These cuts in services for women and babies are likely to have a negative impact on Baby Friendly accreditations. Unicef UK is holding an event for MPs at the Houses of Parliament on December 5th, asking them to pledge their support for breastfeeding. How would it be if every current MP were contacted? Are you willing to contact your MP?
Indicator 9 focuses on national planning for the protection of infants and young children in case of emergency: is there a strategy in place to ensure that suitable nutrition and support is quickly put in place for families in the event of a disaster?
Infants and young children are our most vulnerable citizens in any emergency situation. They need protection, as their immune systems are immature, they have specific nutritional requirements, and they can’t wait several days for an emergency response to meet their needs, especially in a high-risk setting.
Disasters and emergencies in the UK
The UK is not immune from disasters. These can range from storms and flooding, to catastrophic fires and terrorist incidents.
More recently, in response to the arrival of Hurricane Ophelia in Ireland and the UK, the WBTi team has joined in setting up a social media awareness campaign on protecting infants and young children in emergencies, using memes like the one below to communicate key concepts on the Safely Fed UK Facebook page.
Gaps in policies worldwide
Yet around the world, the WBTi global report has found that planning for infants in emergencies is one of the weakest policy areas in infant feeding in many countries.
Global guidance and recommendations
The World Health Assembly (WHA), composed of delegations from all our countries, has recognized the importance of including planning for infants and young children in all disaster-preparedness planning. WHA Resolution 63.23 calls on all nations to incorporate the international standards outlines in the Operational Guidance on Infant Feeding in Emergencies.
The newest update of the Operational Guidance has just been published by the international Infant Feeding in Emergencies Core Group, which brings together leading humanitarian organisations and experts working in this field.
Planning for the protection of infants in emergencies in the UK
The WBTi assessment of UK policy in 2016 found that there is no central national strategy on infant and young child feeding in emergencies, but that emergency planning is devolved to local areas.
(See Indicator 9 on UK policy on planning for infants in emergencies here )
Our first Anniversary Forum, to be hosted by Alison Thewliss MP, chair of the All Party Parliamentary Group on Infant Feeding and Inequalities, at the Houses of Parliament in November, will bring together emergency planners, members of Local Resilience Forums, government agencies, researchers and infant nutrition specialists to explore how protecting infants and young children can be woven into the UK emergency-preparedness system.
In December, the Lactation Consultants of Great Britain will be hosting a specialist training on infant feeding in emergencies in developed countries, led by the Safely Fed Canada team, aimed at public health officials, emergency planners, specialist health visitors working with vulnerable populations and refugees, and infant feeding leads.
Disasters can and do occur in the UK, and we need to be prepared.
Helen Gray IBCLC is Joint Coordinator of the World Breastfeeding Trends Initiative (WBTi) UK Working Group. She is on the national committee of Lactation Consultants of Great Britain, and is also an accredited La Leche League Leader. She represents LLLGB on the UK Baby Feeding Law Group, and serves on the La Leche League International special committee on the International Code.
Support is the theme for National Breastfeeding Celebration Week in England this year. Mothers are sharing their photos and stories of key support from their own “breastfeeding best friend” on social media with the hashtag #bffriend17
Who was YOUR “breastfeeding best friend”? #BFfriend17?
Ruth’s experience is typical: “[Day 6 after the birth, 4am] Me – sobbing: I don’t think this latch is right. It hurts. No, it really hurts. It’s not supposed to hurt. I’m sure it’s not supposed to hurt. But he’s hungry. I have to feed him. I need help. I’m tired, and I’ve got no idea what I’m doing. Who can I get help from?
First time breastfeeding mums the country over will recognise this. The pain of a poor latch, a hungry baby, knowing you need help and not knowing where to get it. At 4 AM, in a state of nearly delirious sleep deprivation. I hung on until the morning, when my dad brought my ex-midwife grandma to help me. She showed me how to relieve my engorgement and soften my nipples so that my baby had something to latch on to. Though it wasn’t totally plain sailing from there. The several days of poor latching had given me a badly cracked nipple, and then I got mastitis. But it healed, and I went on to breastfeed for 2 years. If I hadn’t had my grandma’s support at that moment, I would have stopped breastfeeding.”
So how exactly do we – in England – support breastfeeding mums? There is support available. They can access support from midwives, health visitors, lactation consultants, breastfeeding counsellors and peer supporters. This might be through the NHS, or via third sector organisations such as the Association of Breastfeeding Mothers, the Breastfeeding Network, La Leche League and NCT. (Indicator 6 in the WBTi report, Part 1 and Part 2) There have, however, been significant cuts to many of these services, particularly peer support and drop-ins (part 2, page 30) and there was already a huge postcode lottery in the services available. This is compounded by the fact that there is no national information and communication strategy in England (Indicator 7). There is no centralised database of breastfeeding drop in support (the NHS Choices “find local support” (http://www.nhs.uk/service-search/Breastfeeding-support-services/LocationSearch/360) service uses information held by Netmums) So while there is support available, it can be difficult to find and difficult to access, and in many areas there is just not enough. And it’s certainly very difficult at 4 AM in the middle of a feeding crisis.
Commissioners to ensure there is a range of integrated postnatal services that include both health professional and voluntary-sector breastfeeding support, meet local needs and provide clear access to specialist support.
Government to implement existing NICE guidelines on antenatal and postnatal breastfeeding information and support.
Government to make Baby Friendly accreditation in all maternity and community settings mandatory.
Commissioners to maintain the full range of health-visiting services, and maintain health visiting as a universal service.
Funding for public health to be protected.
PHE to explore options to enable families to access information about local services.
Governments to improve data collection to aid evaluation of services.
Government needs to create a national communications strategy to:
provide accurate information in publications and online sources, liaising more with relevant organisations;
include WBW/National Breastfeeding Celebration Week;
launch a public information campaign aimed at wider society (family, community, workplaces).
DH to update the NHS Choices website to provide accurate information and details of breastfeeding support organisations.
A joined up service which meets the individual needs of each mother is essential to properly support mothers to breastfeed. Different mothers need different levels of support and their needs vary during their breastfeeding journeys. On some occasions an understanding friend is enough, sometimes a peer supporter and on others a highly skilled lactation specialist is needed. When we fail to meet these needs, we fail families. It is time for this to stop. It is time to properly support women in their choice to breastfeed their babies. Who was YOUR #bffriend17?
Post your own selfie with YOUR #bffriend17 on Twitter, Instagram, or facebook!
A #BFfriend can change your life!
Dr Ruth Stirton is a Lecturer in Healthcare Law at the University of Sussex. She works on healthcare regulation, She is an admin of the My breastfeeding Story facebook group and is currently breastfeeding her second child.
If you attended the 2015 Unicef UK Baby Friendly conference you may have noticed, or taken part, in the informal World Breastfeeding Trends Initiative (WBTi) competition to guess the final assessment score. Sue Ashfield is the winner as her estimate was closest to the actual score of 50.5 out of 100 for Indicators 1-10.
The score is a measure of how the UK is performing against the implementation of key policies and programmes to support mothers who want to breastfeed and the healthcare professionals who help them.
Sue is the lead and Specialist Health Visitor (Infant Nutrition) of First Community Health and Care in East Surrey. Sue is a winner in a much bigger way than the WBTi competition because her community team was reaccredited by Baby Friendly earlier this year and they also supported 10 local children centres in achieving full BFI accreditation in one year. The formal presentation of the award was on March 14th. Sue pays tribute to the hard work of her colleagues for the achievement but it also reflects her commitment and leadership. Read more here.
Her team is a brilliant example of what the WBTi UK report recommends for Indicator 6 (community-based support). There is close, integrated working between 0-19 public health team, breastfeeding counsellors, peer supporters and children centres at the three Baby Cafes, which have been runnning for 10 years.
Practitioners from the 0-19 team work at the Baby Cafes on a rota basis, alongside the breastfeeding counsellor. When they see mothers at home or at drop-in clinics they encourage them to attend the Baby Cafes for social support or more specialised support or just to chat to one of the peer supporters. The breastfeeding counsellors at the Baby Cafes have now trained over 200 peer supporters and this has increased the breastfeeding knowledge and skills within the local community.
Credit: Eleanor Stock
The photo above shows Sue holding the Baby Friendly Initiative (BFI) accreditation plaque along with some members of the 0-19 team, some senior managers and their BFI Guardian. Since April, all three community services in Surrey have come together as Children and Family Health Surrey to deliver children’s services.
Sue comments that she found particularly useful the information in the WBTi report about interventions and investment offered in the past and also Report Cards and the summary gaps and recommendations. She will use the findings in the report to inform local commissioners and disseminate information to staff and other stakeholders.
An integrated service like this is needed in all areas, yet in so many places services are being cut, particularly peer support programmes and breastfeeding support drop-ins.
Many congratulations Sue.
Cover photo credit: Paul Carter
Patricia Wise is an NCT breastfeeding counsellor and a member of the WBTi Steering Group
The inspiring story of breastfeeding support in a London borough
What changed?
I have been reflecting recently on my experiences as a specialist health visitor and infant feeding lead in an outer London borough. The story began twelve years ago, in 2005, when there was a lack of confidence among mothers and staff about the reliability of breastfeeding, which was hidden and rarely seen in public. Over the next eight years, the initiation rate increased from 67% in 2005 to 86% in 2013, and the continuation rate at 6-8 weeks from 50% to 75% (52% breastfeeding exclusively). Breastfeeding became the way most mothers fed their babies. Gradually breastfeeding mothers became visible in cafes, shopping centres, supermarkets, streets, GP surgeries and children’s centres. The Unicef Baby Friendly Initiative assessors stated in a report that, in this borough, breastfeeding had become ‘the normal way to feed babies’.
How did it happen?
How did this change come about in a relatively short period of time? It began in 2005, as a joint project between the NHS and NCT, which secured local health authority funding to set up a breastfeeding support group in an area of social deprivation with low breastfeeding rates. This group became very well attended and was facilitated effectively by two NCT breastfeeding counsellors and a health visitor. A similar group was set up in another part of the borough and was run by me, together with other health visitor colleagues. Many of the mothers were very grateful for the support they received in the groups and some of these women expressed the wish to train as volunteer peer supporters, so that they could help other mothers enjoy breastfeeding their babies, as they had. Two training courses were organised and, that year, 20 peer supporters were trained, registered by the voluntary services of the local Primary Care Trust (PCT), and started working in breastfeeding support groups, in the children’s centres and health service clinics. The news of the training spread rapidly and soon there was a waiting list of mothers wishing to train!
Reaching out
The numbers of groups expanded to be easily accessible to mothers across the borough, running every weekday, in children’s centres, cafes, and health premises. The new peer supporters brought fantastic skills with them, one setting up a website, another a mothers’ Facebook page and another designing our leaflets and posters! One had breastfed twins and set up antenatal sessions for parents expecting multiple births plus a weekly support group for mothers with twins and more. She also visited these mothers at home and lent them cushions, which helped them tandem feed. Soon the exclusive breastfeeding of twins and even triplets became common. A group of Somali mothers was trained and an outreach peer supporter started seeing Somali pregnant women in the hospital. A teenage ‘buddy’ scheme was also started by some of the younger peer supporters, working with the specialist midwife and running antenatal sessions and postnatal support for young mothers. Two peer support co-ordinators were employed to job-share this important role and to deal with concerns of the peer supporters as well as helping with training and supervision. Over the next ten years, more than 200 voluntary peer supporters were trained in the borough and the training continues until the present day.
Unicef UK/Mead
Public Health prioritises breastfeeding
In 2006, under the government scheme of “Every Child Matters’, the Director of Public Health made breastfeeding the top priority for all children in the borough with accompanying ‘stretch targets’ and funding.
London services are monitored through the ‘Good Food for London’ report on their Baby Friendly status, with details on how each borough is achieving and sustaining the Baby Friendly standards
Baby Friendly accreditation
In 2012 Unicef UK Baby Friendly Initiative carried out a major review that resulted in new, more holistic, child rights-based standards relating to the care of babies, their mothers and families, with a strong emphasis on building responsive loving relationships. A new award has also been introduced to encourage a focus on sustainability after the accreditation.
In parallel with the rapidly increasing numbers of peer supporters, the journey in the borough to become Unicef Baby Friendly (BFI) accredited started and professional training in the community and local hospital began with the two health trusts starting their journeys jointly. A model of multidisciplinary training of midwives, maternity assistants, neonatal nurses, nursery nurses and health visitors began initially with BFI-facilitated training. This enabled hospital and community staff not only to improve their breastfeeding knowledge and skills, but also each other’s roles, co-operate on work challenges and break down any barriers which may have existed previously. Communication skills and talking about their own life experiences, in order to gain an understanding of their impact, especially with infant feeding, became an important part of the in-service training. Interactive group exercises on different breastfeeding situations became an integral part of the training, emphasising the importance of empathy and seeing the problems through the eyes of the mothers. A neonatal breastfeeding co-ordinator was appointed and started training all the neonatal staff in the hospital, including the doctors, and by 2014, Unicef had awarded both the community and hospital trusts their Baby Friendly accreditation.
Peer support
Peer supporters were also employed by an adjacent borough to work in the hospital, supporting mothers on the postnatal ward, one even working all night once a week; others taught hand expressing and colostrum harvesting in the antenatal clinic, especially for mothers with diabetes.
Unicef UK/Mead
Achieving cultural change
Within ten years, breastfeeding became a normal and accepted way to feed babies in the borough. Mothers, fathers, and grandmothers-to-be came in large numbers to the twice monthly breastfeeding workshops, gaining confidence and information, with the expectation of the support that would be available to them to help them achieve their goals. A mother said ‘the session expelled myths and I now know how milk is made and transferred to my baby. I am looking forward to skin-to-skin contact after the birth and will follow my baby’s instincts’. Parents meet peer supporters in the support groups, at toddler groups, in the school grounds, in cafes, at sports events, in churches, temples, synagogues and mosques. Peer supporters live and work in the community and spread their knowledge through everyone they meet. Even when they move away from peer support, they take their embodied knowledge into the work place and support their colleagues there. Cultural change can happen through peer support, resulting in breastfeeding becoming embedded in a community. This change is sustainable over time and in future generations, as it spreads through different social groups. Voluntary peer support and informed, professional support is capable of changing attitudes and behaviour within a community to make breastfeeding ‘normal’ in a very cost-effective way. Commissioners need to be aware of how health outcomes can be improved through breastfeeding, for mothers and children, in the immediate and long-term, and it is essential to protect and increase future funding for midwives, health visitors and peer supporters, in order that vital programmes like this can continue.
The World Breastfeeding Trends Initiative UK report in 2016 affirmed the borough’s actions as it recommends in Indicator 6 (Community-based support) that ‘commissioners ensure that there is a range of postnatal services that include both health professional and voluntary-sector breastfeeding support to meet local needs and provide clear access to specialist support’ and that they ‘maintain the full range of health visiting services, and maintain health visiting as a universal service’. Indeed, the borough’s transformation in breastfeeding support is used as a case study in Part 2 of the report.
One mother with an eight-month old baby told me:
‘I so much wanted to breastfeed, but found it incredibly hard at the beginning. I was convinced that it wouldn’t work and it was such a lonely feeling, like I was failing where other mothers were succeeding. Getting support made all the difference- having someone to listen to me and give me confidence to carry on. Suddenly, I didn’t feel alone any more and it changed everything. I know that I would not be breastfeeding now if I hadn’t got help in those crucial first weeks.’
What one London borough has achieved shows what is possible. Unicef UK Baby Friendly Initiative’s Call to Action spells out four key actions to create a supportive, enabling environment for women who want to breastfeed, ranging from national strategy and legal protection from harmful commercial practices to the local implementation of evidence-based practices, as described
This week, support is the theme of Breastfeeding Celebration Week
#bffriend17
There’s so much to celebrate about breastfeeding, and for me one of the most special things is how much we can learn from each other as mothers.
Of course there is information everywhere, often far too much of it, and there are medical professionals to give technical support, check our babies’ health, and prescribe any treatments that are needed. But in my time as an LLL (La Leche League) Leader, I’ve noticed that passing on pure information is a tiny part of what we do. What brings mothers to our meetings, and turns them into loyal regulars, is the talking – the chance to share their strong feelings about their unique developing breastfeeding relationships.
The simplest of questions: “how do you know when your baby wants to nurse?”; “what surprised you most about breastfeeding?” can easily set off half an hour of discussion. Dazed new mothers with tiny newborns share their shock and wonder; seasoned mothers on their third child talk about how still, every day, there’s something new.
And of course mother to mother conversations like these provide a safe space for complaining. As one mother put it to me: “LLL meetings are the only place where I can sit and moan about breastfeeding without being instantly told to wean”. When a group starts from a safe shared understanding that breastfeeding matters, and a shared knowledge of its many joys, this gives a context that makes it acceptable to explore the lows, too.
The support of peers can also give a rich source of alternative methods and ways to approach breastfeeding-related problems. A mother suffering through a nursing strike can find a “standard list” of solutions online easily, but there’s a whole extra dimension when she can describe it to other mothers who are right there with her. She can show her child other busily nursing babies, and can talk about any mixed feelings she has – perhaps she’s wondering if this might be a chance to wean that she’ll later regret not having taken, or she might be wondering what effect this will have long term on their breastfeeding relationship. Finally, she might return to the next month’s meeting glowing with happiness as she and her baby are back in tune, all is well, and she has added to her stock of experiences to share with the next mother.
Support from medical and lactation professionals has a crucial place; in times of serious need, specialist help from a lactation consultant can be literally life-saving. And sometimes, in the middle of the night, reaching out to strangers on the internet can be enough to get through.
But for everything else, there’s mother to mother support. It’s embedded in its community, and forms a community of its own within that. Mothers come to LLL meetings nervous, uncertain, clutching newborns and wondering what to expect; sometimes they’re still with us years later, bringing all their successive children, perhaps becoming LLL Leaders themselves, or perhaps just carrying on the conversation, and passing on the support to new versions of themselves.
#bffriend17
To recognise the importance of support, mothers are invited to share their photos and stories of support from their own “breastfeeding best friend” on social media, using the hashtag #bffriend17.
Post your own selfie with YOUR #bffriend17 on Twitter, Instagram, or Facebook!
Editor’s note:
You can find the findings from the WBTi assessment of mother support in the community in “Indicator 6” in our 2016 report
With further details on mother support in the community in Part 2
Helen Lloyd is a Leader with La Leche League GB, and fits in as much time supporting breastfeeding as she can around the needs of her own young children
I received too much breastfeeding support – said no mother ever!
Your vibe attracts your tribe
#BFfriend17
I did not realise the power of that statement until I became a breastfeeding mother. Nursing my child became a life philosophy, a kaleidoscope lens, spinning my family, bringing like-minded people together and painting the colours of my parenting. About 3 years ago there was a story all over the media about a mother who was asked to leave a certain store because she chose to breastfeed openly in there. Breastfeeding mothers on social media were furious. Simultaneous protests in branches of that store were set up and I organised one of them. Some great friendships were born out of that movement. This simple act sparked a discussion about the needs of the breastfeeding community. This could not end there.
Protest was the beginning.
We wanted to make sure mothers knew their rights. We wanted to educate, empower and bring families together. Slowly a community has been born. It kicked off with a picnic to celebrate National Breastfeeding Week, followed by some meetings in a children’s centre. A year passed and having my third baby gave me a huge boost of confidence to put my peer support training into practice. After another season of outdoor gatherings, I hired a room in a community centre. One of the mothers got inspired and started another group in a nearby town, followed by more of them. All were hosted by mothers who breastfed their own babies and felt they could support others and offer a safe space for befriending.
A few months later we decided to organise peer support training. The services offered by the local health visiting team and children’s centres were not sufficient at the time. And there definitely was a niche for peer support. Having experienced first hand how unique it is having another mother support you through hardships, I fell in love with the idea. We approached other service providers using the Maternity Services Liaison Committee. At first, not many believed in us but, as time passed, we proved to be worthy of their trust. We asked for help from generous friends, who delivered the training at no charge, and we found a venue for free thanks to a children’s centre manager. But mostly we were incredibly lucky to recruit, through our groups, amazing women who agreed to offer their time to volunteer in the local hospital.
We decided it was the right time to create something more formal. West Herts Breastfeeders community came to life thanks to the many mothers who nurtured it deeply. This ‘baby’ was very lucky. It was a firstborn who had all the attention and support from local Infant Feeding teams and the Children’s Services department of Hertfordshire County Council. We came a long way. It took us just over a year to train 18 peer supporters, establish six monthly regular meetings in the West Herts area, recruit nearly 550 members to our virtual community to provide them with 24 hour support through Facebook and all that with no official funding. We are all volunteers. You could be too!
Be the Change
As mentioned in the Open Letter of February 2016, organised by the WBTi UK team, a woman’s ability to breastfeed is often determined by the support she receives and the environment in which she lives. While we cannot change everything, we try to help normalise breastfeeding out and about. We also play an important role in normalising feeding older babies and encouraging mothers to carry on, while often dealing with family pressures to wean or the challenges of returning to work. Most children’s centres provide breastfeeding support only in groups for babies under one year, and health visitors do not see mothers as often as they would like. Not having a healthcare professional label also changes the balance of the dialogue and helps mothers to open up.
Together we can do more
What we strive for in the face of recent cuts and challenges is the partnership between all local services. Our success is owed largely to the power of networking. We can see where we are needed most and what else can be done to make sure no woman is left alone at any stage of her nursing journey. You can help to be part of the change, by simply sharing your thoughts with your newly elected MP. Use the WBTi sample email to tell them what breastfeeding mothers need in your local area. Ask them to use their influence on the Local Authority to showcase the importance of breastfeeding to public health and safeguard their budget for health visiting and breastfeeding support.
Your voice matters.
Please sign up HERE to receive email updates on our WBTi work!
Bio
Olga Danyluk –Singh, Chairperson, West Herts Breastfeeders
NHS Breastfeeding Peer Supporter and mother of three breastfed children
I imagine like me you have watched some pre-election television debates in the last few weeks. It’s easy to start daydreaming and picture yourself in that audience putting our leaders on the spot. If you had the opportunity to ask that one key question of the main political leaders and get it broadcast on national television, what would you choose to focus on?
For many of us who have been involved in the WBTi project, it’s a no-brainer: What would they do to improve the situation around breastfeeding and infant feeding in the UK?
Except you’ve only got one sentence to outline a situation that took WBTi more than 70 pages.
You’re talking about health care professional training and the international code of marketing of breastmilk substitutes, national leadership, maternity protection in the workplace, data collection. Plus, you are talking to people who don’t even realise there is a problem in the first place or have little understanding of the complexity. There are few soundbites developed for an issue that affects families across the UK and for a situation that many of us see is in crisis.
Breastfeeding is a public health imperative
Politicians are nervous to touch on an issue which they often see as being about individual choice rather than a ‘collective societal responsibility’, as Dr Nigel Rollins described breastfeeding in The Lancet report last year. But when you look at the reality of what is happening in the UK, there is no need to fear having a conversation about breastfeeding. It’s not controversial to be disappointed to hear that 86% of women who stopped breastfeeding in the first two weeks would have liked to have continued for longer. Or 63% of those who stopped before 10 months. It’s especially not controversial when you learn more about the impact of breastfeeding on maternal mental health and its role in reducing inequality.
Which politicians wouldn’t be interested in something UNICEF describe as ‘a natural safety net against the worst effects of poverty’ or a factor shown to have a significant impact on the national economy? We can read through the manifestos of the political parties and see references to obesity and child health and mental health and find ourselves exasperated that infant feeding hardly gets a mention. However, it IS there. In every discussion about fighting inequality or improving chances or protecting the environment or stimulating the economy or supporting parents or focusing on mental health. They just don’t KNOW it’s there.
It is our duty to get this message across.
We may not be sitting in a Question Time audience but we meet our candidates. We have their emails and Twitter accounts. We can speak to them once they are sitting MPs.
Use the WBTi sample email and add your own messages to all the candidates in your own area. What are the gaps in breastfeeding services in YOUR area? Tell YOUR story.
It’s about emphasising why funding matters and why breastfeeding support in the community isn’t a nice optional extra. We are hearing about the huge variation in community-based support across the UK. Cuts to services in England are particularly a worry. Parents are finding groups closing, peer support services disappearing and when they are struggling with more complex problems, there is often nowhere to go. Specialist positions are either being lost or the integration of services means signposting to more qualified breastfeeding specialists such as IBCLCs is confused.
There is no point sighing about the crisis in infant feeding unless we also act. No point in putting a nice meme on your social media account, without also making sure you take 5 minutes to educate a politician who may simply not understand the basics. No point having anger towards our leaders if they are uninformed. WE are the ones who can do the informing: the new parents, the breastfeeding organisations, the healthcare professionals. It’s all too easy for social media to become a place where we all just talk to people who already agree with us. It has never been easier in history for us to directly contact our candidates and politicians. They won’t understand these issues unless we educate them. It starts with one email or one tweet or one conversation.
Have you done it?
For more information about cuts to community breastfeeding services, see WBTi’s 2016 briefing
See the Open Letter signed by dozens of royal colleges, health professional bodies, researchers and voluntary organisations
Responses from political parties
Baby Milk Action have asked all the major political parties about their breastfeeding and infant feeding related policies. You can read their letter, which refers to the WBTi UK report, and the responses they have received here.
Photo credit: Sophie Burrows
Emma Pickett IBCLC is Chair of the Association of Breastfeeding Mothers. She is also an ABM breastfeeding counsellor (www.abm.me.uk) in North London. She has supported breastfeeding mums in Haringey as a volunteer since 2008.
‘I’m still not convinced breastfeeding 4 year olds should be considered normal!’ – feedback from final year medical student after teaching session
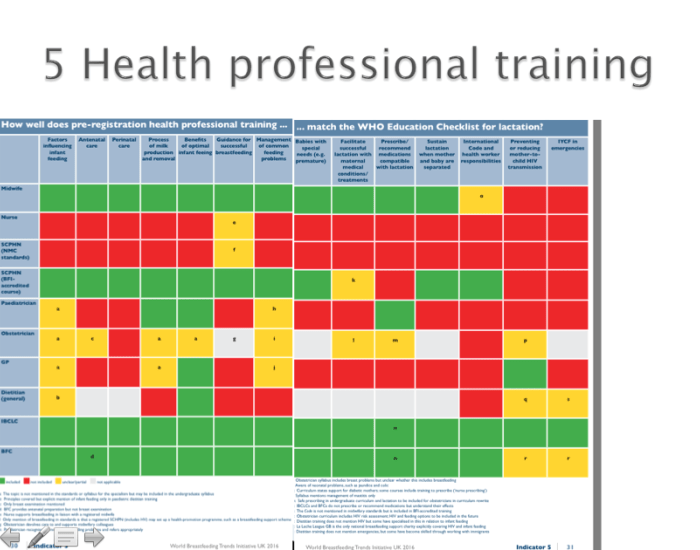
‘Most [UK] pre-registration training for healthcare practitioners who work with mothers, children and young infants has many gaps in the high-level standards and curricula…’ World Breastfeeding Trends Initiative report 2016
As a consultant paediatrician, I deliver a one hour seminar to our medical students several times a term. I have the coveted before-home time slot for ‘essentials of paediatric nutrition’, which aims to encompass the investigation and management of faltering growth, the aetiology and treatment of obesity, and all infant feeding issues. Luckily I talk fast.
Of course, I’m joking. Covering the syllabus in that time means focusing on key points, and one way I try to do this is encourage the students to set the agenda. At the start of the seminar, I plot out on a whiteboard what they want to get from the session. The students always ask me to cover the different types of formula. In fact, their syllabus emphasises breastfeeding, but their preoccupation is with learning components of, and indications for, breastmilk substitutes. This is manageable rote learning, standard in undergraduate education, easy to put on a flashcard and commit to memory for exams. It also connects to the overwhelming societal perception that formula is the default feed for babies. It is much harder to open up a discussion about breastfeeding and accept that we, as doctors, know almost nothing about it because we aren’t seeing it or learning about it at medical school. Of the twenty or so students in each session, often only one or two have seen a baby breastfed at all. Usually no one in the room has seen a child over the age of one nursing.
The ignorance around breastfeeding continues into our postgraduate curriculum. The ‘breast is best’ message is emphasised (although that has been superseded elsewhere by the ‘breast is normal’ message) but without the backup of grounding in lactation physiology and how our profession contributes to what I think of as ‘iatrogenic low milk supply’ – medical practices such as separating mother and baby, delaying the first feed, not respecting the importance of skin to skin, feeding on an artificial schedule, wrongly assuming that maternal and infant medical conditions and medication preclude breastfeeding… Without understanding the science, doctors will always resort to what they have seen before, are comfortable with, and believe to be normal. At the moment, that is usually formula feeding.
The World Breastfeeding Trends Initiative report flags up the holes in training for healthcare practitioners – illustrated here, the universal minimum pre-registration standards set by the GMC, the NMC and the BDA – and my experience echoes that (see Indicator 5, in Part 1 and Part 2, online). Our doctors need to realise what they don’t know about breastfeeding before they can start to learn. Recognising this is the first step on a very long road, but it is at least a step forward.
Dr Vicky Thomas is a consultant paediatrician at the Great North Children’s Hospital in Newcastle upon Tyne. A generalist at heart, she has developed an interest in growth and nutrition and is passionate about the role of breastfeeding in optimising child health.
























 Emma Pickett IBCLC is Chair of the Association of Breastfeeding Mothers. She is also an ABM breastfeeding counsellor (
Emma Pickett IBCLC is Chair of the Association of Breastfeeding Mothers. She is also an ABM breastfeeding counsellor (


{kind=link}